Abstract
Metastatic colorectal cancer at a young age with a pre-existing congenital colorectal motility disorder is a rare but serious presentation. We wish to present an unusual and interesting young adult male who presented with a metastatic colonic carcinoma. Patient had past history of congenital motility disorder, for which the patient was investigated with a battery of studies during infancy and childhood and treated intermittently when symptomatic. During current admission investigations for right upper abdominal pain and diarrhea with possible cholelithiasis or cholecystitis, the patient was found to have multiple liver metastatic lesions from the right colon cancer at the hepatic flexure. Palliative and rehabilitative treatment with diverting ileostomy and chemotherapy was offered, but succumbed in six months with further rapid progression of the undifferentiated metastatic colon cancer.
Introduction
Colorectal Cancer (CRC) is the 3rd most common cancer in men and the 2nd in women globally, while its presentation in patients below 40 years is rare [1]. Early-onset colorectal cancer (EOCRC) refers to CRC diagnosed in individuals under 50 years old. It is a distinct entity with increasing incidence globally, especially in high-income countries. While the exact reasons for the rise are still being investigated, factors like lifestyle changes, obesity, and potential genetic predispositions are being explored. EOCRC often presents with more advanced disease and has different molecular characteristics compared to late-onset cases. Similarly, conditions like Hirschsprung’s disease or other congenital or acquired motility disorders are more prevalent, difficult to diagnose, and challenging clinical entities. It can cause chronic constipation, alter bowel habits, and potentially increase the risk of EOCRC development, although the exact relationship is still under investigation. We present our experience with a case of EOCRC recently encountered. The aim is to highlight the possible role of unrecognized under-recognized mild congenital colorectal disorders as a predisposing factor, and object is to suggest potential change in the criteria in current referral pathways in view of changing EOCRC and to review the criteria for promotion of health, prevention, early detection, cure, etc.
Case Presentation
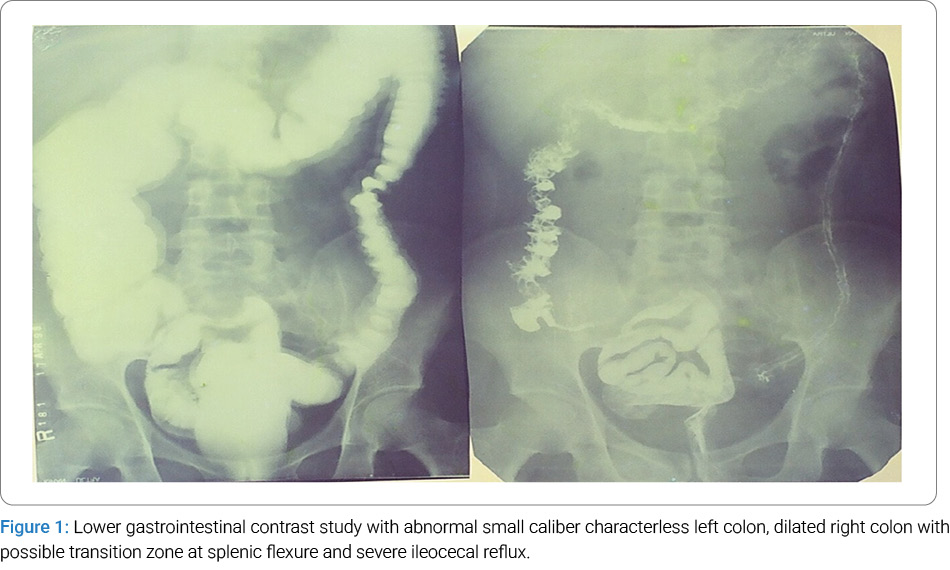
A 34-year-old male developed intermittent right upper quadrant pain, abdominal bloating with increasing constipation, in the background of chronic loose stools, and was referred by a general practitioner for possible cholelithiasis investigations. The patient was born at term and passed meconium at birth immediately, but developed chronic constipation in late infancy, and a rectal suction biopsy had suggested few ganglion cells with no nerve hypertrophy, and acetyl cholinesterase staining was normal. A full-thickness rectal wall biopsy with anorectal myomectomy was advised to rule out ultra-short-segment Hirschsprung’s disease, which was refused by the parents. Patient had escalation of bowel symptoms together with adolescent nonspecific urethritis symptoms during the teenage period, and a lower gastrointestinal contrast study revealed characterless small caliber left colon with loss of haustra with a possible transition zone at the splenic flexure, dilated transverse and right colon together with massive ileocecal reflux on filling and post-evacuation radiographs (Figure 1). Patient had been treated in the past for chronic constipation, dairy and gluten intolerance, acute and chronic anal fissures, mild rectal mucosal prolapse, intermittent bleeding piles, irritable bowel syndrome with alternating constipation and diarrhea as independent symptoms and previous investigations never qualified him for 2 weeks wait or an elective gastroenterology referral as the routine screening investigations never indicated any specific persistent progressive abnormality. The patient responded well to conservative management at each individual episode of clinical presentation for a significant period of time. There was no family history of any bowel cancers or other cancers. The patient had no bowel symptoms in the past 5 years preceding the current presentation. In addition, the patient had severe psychosomatic and socioeconomic stress, low-fiber, high-fat diets high in processed meats and foods, a sedentary lifestyle, obesity, smoking, and heavy alcohol use as additional risk factors.
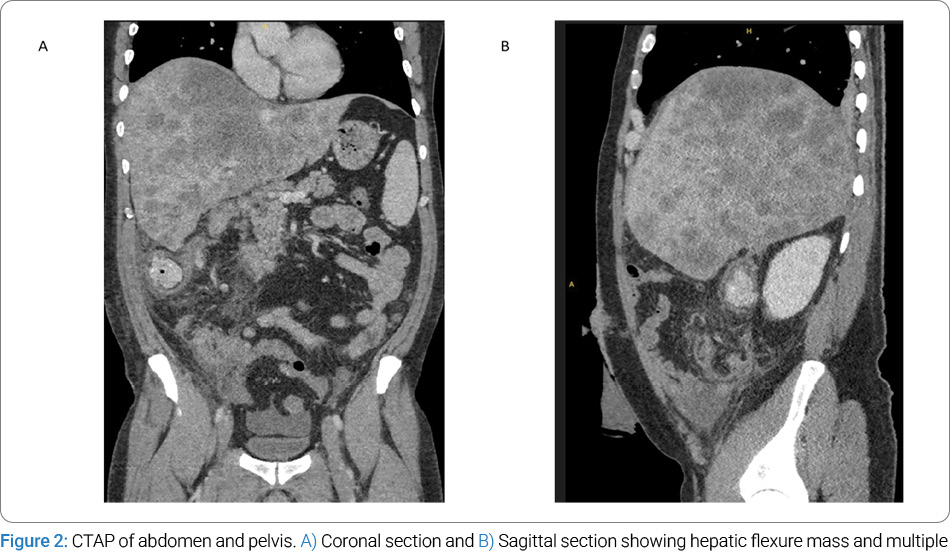
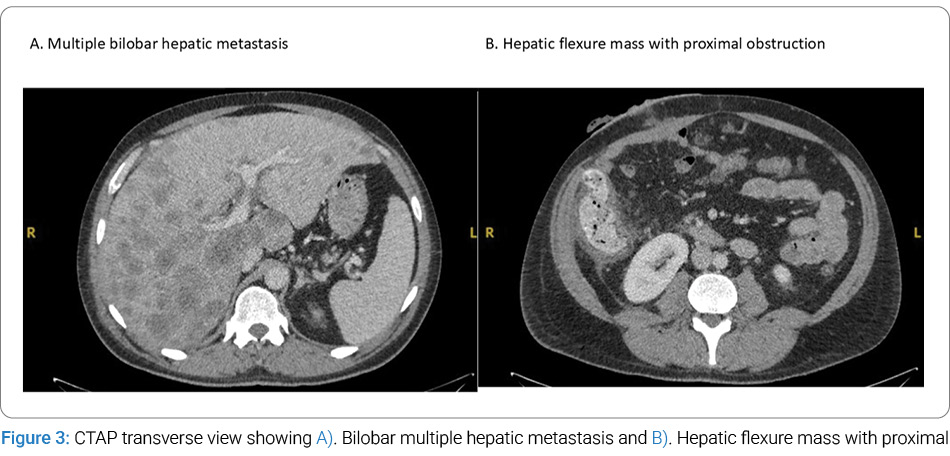
Laboratory investigations were normal except for abnormal liver function tests. Abdominal ultrasound showed multiple liver metastases in both lobes with a hepatic flexure mass in the colon. Computed Tomography of Abdomen and Pelvis (CTAP) with contrast study confirmed multiple bilobar hepatic metastases together with an obstructing mass in the hepatic flexure of the colon in the coronal and sagittal views (Figure 2) and transverse sections (Figure 3). A transcutaneous fine needle aspiration biopsy of liver metastasis confirmed highly undifferentiated signet ring metastatic colon cancer.
The patient was referred to the genetic team and had an appointment with them in a few weeks’ time, which was attended by the patient with a detailed family pedigree and analysis, which indicated no hereditary syndrome or family-related genetic issues, but a mutated gene was strongly suspected to be a gene mutation. The test was not available locally, and the patient did not have enough resources to afford it privately, so it could not be performed.
At a multidisciplinary meeting, palliative chemotherapy and diverting ileostomy were decided, which he underwent uneventfully. The disease progressed unremittingly with lung metastasis, and he succumbed in the six-month period since diagnosis. The family members and friends had concerns regarding the delay in diagnosis by the general practitioners or earlier physicians regarding the possible errors of technique or judgment. The background of ongoing bowel symptoms since early infancy, with a missed pseudo-Hirschsprung’s disease, or whether early referral would have made any difference. The multidisciplinary team counseled them, and they went through the whole process. At no stage did he qualify for any urgent or routine referrals as per the existing criteria and the way the patient has responded. There was no events where a persistent symptom, sign, or test remained abnormal. a no-blame strategy was applied, and the family was reassured that we will make every effort to improve the awareness of the underlying, unrecognized, and untreated congenital bowel disorders in the pediatric specialists and possible change of referral criteria for the adult patients.
Discussion
Our extensive experimental, transitional, and clinical research indicates that the congenital colorectal motility disorder is more prevalent than recognized, has very subtle symptoms and signs, with the patient looking apparently healthy with its partial functional bowel obstruction, and have very strong potential to predispose to gut-related and extraintestinal diseases and manifestations later on in life with far-reaching consequences. On the other hand, the diagnostic challenges for EOCRC remain. Younger patients may present with vague or atypical symptoms, and there may be a lower initial suspicion for CRC, leading to delayed diagnosis and potentially more advanced disease at presentation. The rising incidence of EOCRC is raising concerns about the disease’s impact on public health.
The truth is, EOCRC has been on the rise for years. A patient can have colon cancer for a number of years without knowing because early symptoms can be vague and subtle. Time to develop a classic colon cancer may take 5–10 years for a polyp to develop into colon cancer in the traditional late onset CTC, but EOCRC can have very fast growth, and it spreads so rapidly like wildfire, making their survival rates difficult and challenging. However, recent research has identified that the EOCRC has distinct clinicopathological differences with the older patients and some specific key aspects of pathology [2], and another recent study showed a high incidence of EOCRC at a more advanced stage of disease. Mucinous type and signet ring cell carcinoma of the colon are poorly differentiated and present at an advanced stage than non-mucinous adenocarcinomas [3].
In the early stages, there may be no symptoms, or they may be confused with an underlying colorectal motility disorder. Symptoms may include blood in the stool, changes in bowel habits, such as diarrhea or constipation, abdominal pain, weight loss, a persistent urge to have a bowel movement and pale stool. The treatment for older patients with colon cancer is complex due to factors such as comorbidities and geriatric syndromes, particularly frailty while the EOCRC patients are having more aggressive cancers and due to late advanced disease presentation may not be suitable for major radical surgical interventions [4].
Potential risk factors include lifestyle factors, such as a westernized diet, obesity, physical inactivity, and increased antibiotic use, which are hypothesized to play a role; genetic predisposition, with hereditary cancer syndromes like Lynch syndrome are also linked to EOCRC and other factors, including alcohol consumption and processed meat intake, which are also associated with increased risk. Research has shown that one in five patients with early-onset CRC has at least one pathogenic susceptibility gene mutation, representing a higher percentage compared to late-onset CRC [5]. Colon cancer is a very common and serious disease that warrants prompt medical attention. Promotion of health and prevention of Colon cancer is a very common and serious disease that warrants prompt medical attention. Promoting health and preventing colon cancer is the master key; failing which, early detection and appropriate treatment are the keys to success. If any individual has any change in their bowel habits-constipation and/or diarrhea or both alternating, if they have any bleeding—even if they think it’s a hemorrhoid, and it doesn’t go away—just get a colonoscopy and biopsies to detect the colon cancer early and treat it appropriately [6].
However, even though recently CRC is rising in young people, the overall incidence is still too low to justify routine colonoscopies for them. Once a screening test is developed for a disease, it’s important to make sure that the number of screenings performed will prevent enough cancers to justify the costs of and risks associated with the tests. Rectal examination and proctosigmoidoscopy or limited left colonoscopy has no role in right sided colon cancers.
EOCRC exhibits distinct molecular characteristics compared to late-onset CRC, including higher rates of microsatellite instability. The progression of colon cancer varies according to the genetic predisposition, cellular makeup of the tumor, differentiation, stage of the disease, age and sex of the patient, and other factors. Additionally, the issue of early age screening introduction, which allows early diagnosis of the disease, is also important; the younger population is not included in current existing programs, except for the highest-risk groups. If the phenomenon of early age CRC becomes more prominent, screening programs will have to be reviewed, but with consideration of the consequences for health economics [7].
Treatment for metastatic CRC in young adults is similar to that of older patients, involving chemotherapy, surgery (if possible), and targeted therapies. However, the prognosis can be more challenging due to the advanced stage at diagnosis and potential differences in tumor biology. EOCRC may have a genetic predisposition and be linked to hereditary cancer syndromes or specific genetic mutations. Testing for these syndromes should be considered.
Understanding the molecular profiling and characteristics of the tumor (e.g., microsatellite instability, CIMP status) is crucial for guiding treatment decisions and potentially identifying targeted therapies. Management of metastatic EOCRC requires a multidisciplinary team, including oncologists, surgeons, gastroenterologists, and genetic counselors. Globally, research studies on CRC have documented distinct differences in disease characteristics of younger and older patients in terms of stage, grade, location of tumours, and survival. The EOCRC patients present with a more aggressive disease, are advanced in stage with unfavorable histopathological findings, especially mucinous and signet ring cells [8–12].
Conclusion
Our case is a useful reminder of the fact that although CRC in young adults is rare and scary, it highlights the importance of early detection and awareness of CRC in young adults, especially those with underlying conditions that may affect bowel function. The case emphasizes the need for healthcare professionals to maintain a high index of suspicion for CRC in young adults, especially those with a history of bowel dysfunction. Symptoms like persistent changes in bowel habits, unexplained weight loss, or abdominal pain should be investigated promptly. In summary, this presentation underscores the importance of increased awareness and vigilance for CRC in young adults, especially those with underlying bowel conditions. Early diagnosis and tailored treatment are crucial for improving outcomes in this challenging clinical scenario. The rising incidence has prompted discussions about lowering the recommended screening age for CRC.
Conflicts of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
Cite this article
Patel RV, Govani DR, Swamy KB, Midha PK, Govani ND, Panchasara NG, et al. Metastatic colonic cancer at presentation in a young adult with a background of congenital colorectal motility disorder. Clin Case Rep J. 2026;7(1):1–4
Keywords
Congenital colorectal motility disorders; Pseudo-Hirschsprung’s disease; Ileostomy computed tomography; Young age; Hepatic metastasis
Copyright
© 2026 Ramnik Patel. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
