Abstract
Objective: This investigation endeavors to scrutinize the most potent evidence for the prevention of Device-Related Pressure Injury (DRPI) and incorporate it into clinical practice, subsequently analyzing its outcomes.
Methods: A total of 36 articles of orthopedic DRPI-related evidence based on the SSKINS cluster management model in the initial phase were chosen, and examination standards encompassing 14 indicators were formulated, and the nursing practice was clinically evaluated according to these criteria. Through the analysis of its evaluation results, we compared the discrepancies in nurses’ DRPI knowledge and conduct level, review index implementation rate, and the comfort and patient’s Visual Analog Score (VAS).
Results: The incidence of DRPI diminished from 19.67% (12/61) to 3.07% (2/65); the nurse’s preventive DRPI questionnaire score escalated from 92 to 62 (78.31 ± 5.77) points at the initial review time to 86 to 100 (88.31 ± 3.77) (t = 5.867, P < 0.001); the patient’s VAS score was reduced from 2.0 points in the initial review time to 1.81 ± 0.39 points (P < 0.001); patient PCS-C comfort score increased from 40.31 ± 3.85 points in the initial review time to 44.82 ± 2.67 points (P < 0.001); Prior to the utilization of evidence, the clinical implementation rate of 14 review indicators ranges from 0 to 100%, with the implementation rate of indicators 4, 5, 6, 12, 13 and 14 being < 70%. Following the application of the evidence, Indicator 4 utilized the “Orthopedic DRPI Risk Assessment Form” for risk assessment, and Indicator 12 Nurses conducted DRPI education to patients and issued DRPI prevention guidance manuals. The implementation rate of the review index was elevated from 0% to 100%; Indicator 5 patients with complex trauma utilized customized splints or orthotics, Indicator 6 patients utilizing instruments utilize protective pads or preventive dressings, Indicator 13 patients are aware of the pertinent contents of the instrument, Indicator 14 nurses employ VAS and PCS-C to evaluate patient comfort daily. The implementation rate of the review index has been raised to over 95%.
Conclusion: The application of the most efficacious evidence of orthopedic instrument-related stress damage based on the SSKINS cluster management model has catalyzed the enhancement of the knowledge level of medical staff to prevent DRPI and the modification of behavioral norms, and mitigated the risk of pain and stress damage in patients.
Introduction
Medical devices are external risk factors for the development of Pressure Injury (PI), and medical devices that directly or indirectly touch the skin will increase the risk of PI [1,2]. In 2016, the US National Pressure Ulcer Advisory Committee formally proposed the concept of medical device-related Pressure Injury (DRPI) and defined it as “a stress injury caused by the use of a medical Device designed and applied for diagnostic or therapeutic purposes” [3]. Unlike traditional PI, DRPI is usually caused by diagnostic or therapeutic medical devices, and the damage is typically consistent with the device’s design or shape. Studies have shown that the incidence of DRPI in foreign countries ranges from 3.10% to 26.70%, accounting for about 1/3 of PI in hospitals [4]. A survey in China showed that the incidence of DRPI in ICU patients was 1.65%, accounting for 43.50% of device-related stress injuries in hospitals [5]. Orthopedic instruments are used with high frequency and for long periods and long home nursing stays, and orthopedics has become one of the most popular departments for DRPI. In strict accordance with the evidence-based nursing method, the evidence-based team formulated the best evidence for the prevention and management of orthopedic device-related stress injuries in the early stage, and carried out the transformation of evidence to the clinic in accordance with the four stages of “continuous quality improvement of evidence”, evidence acquisition, clinical status review, evidence introduction, and effect evaluation. Based on SSKINS (S-Skin, S-Surface, K-Keep moving, I-Incontinence, N-Nutrition, S-Selfcare) cluster management model, Structured nursing interventions include six aspects: skin, supporting surface, activity, excretion, nutrition, and self-care [6,7]. Therefore, this study applied the method of clinical quality review, first reviewed the current situation and then introduced the evidence, analyzed the obstacle factors of evidence in clinical practice, and formulated improvement countermeasures to prepare for the introduction of the best evidence into the clinic, with a view to building a standardized process for the prevention and management of orthopedic device-related stress injuries and guiding the clinical work of nurses.
Methods
This study adheres to the seven-phase JBI Evidence Implementation Framework. Project execution comprised seven steps: 1) identifying the need for change, 2) engaging change advocates, 3) assessing context readiness, 4) assessing current practices against evidence-based criteria, 5) implementing changes, 6) reassessing practices post-implementation, and 7) examining sustainability. The preparatory phase encompassed theoretical preparation, PIPOST construction, evidence extraction, evidence quality critique, and evidence synopsis. The implementation phase encompasses creating review indicators, conducting impediment analysis, developing a modification strategy, motivating through leadership, and establishing facilitative factors. The evaluation phase comprises design execution study and gauge outcome index; The preservation phase encompasses designing execution studies and gauging outcome indicators. Evidence-informed nursing methodologies were employed to summarize the optimal evidence of orthopedic device-related stress injuries in orthopedic patients, formulate evidence-based practice blueprints, and implement them in the Department of Orthopedic Surgery of a Grade-III hospital in Wuhan from May to August 2024, following baseline review, analysis of impediment factors, and construction of the optimal evidence application strategy. The indicators of patients prior to and subsequent to the application of evidence, and the implementation rate of the review indicators, were contrasted.
Intervention Implementation Details: The evidence-based intervention was implemented comprehensively based on the SSKINS model. Training for nurses encompassed: 1) Theoretical instruction on DRPI concepts, pathophysiology, risk factors (mechanical, device, patient-related), and common sites/instruments in orthopedics; 2) Hands-on demonstration and practice for using the ‘Orthopedic DRPI Risk Assessment Form’, skin assessment techniques (including visual inspection and palpation under devices where possible), correct application of protective dressings (hydrocolloid, foam), padding techniques, and device repositioning; 3) Education on patient communication strategies for conducting DRPI health education and comfort assessment using VAS/PCS-C scales. Standardized Operating Procedures (SOPs) were developed for key interventions: DRPI risk assessment within 8 hours of admission and after device application, skin assessment frequency (at least twice daily, more frequently for edematous patients), application criteria and techniques for different preventive dressings, and the protocol for bridge/pontoon fixation of tubes. Supervision was conducted by the ward head nurses and the six quality control nurses. They conducted weekly audits of nursing records to ensure completion of risk assessments, skin assessments, and documentation of interventions. Random spot checks were also conducted to observe compliance with the assessment and intervention protocols in clinical practice. Feedback was provided during weekly departmental meetings.
Implementation planning:
Phase 1: Identification of practice area for change.
This study elected the orthopedic ward of a premier-tier hospital in Wuhan as the research focus, encompassing nurses involved in evidence implementation, orthopedic adult patients receiving apparatus fixation, and system resources related to the systemic process, ambiance, and equipment of the orthopedic ward. The department boasts a total of 47 beds. This project was executed in the Department of Bone Surgery of a Grade III Hospital in Wuhan from May to August 2024. A total of 61 patients at the initial review from May to June 2024 and 65 patients after the application of optimal evidence from July to August 2024 were selected as study subjects using convenience sampling.
Phase 2: Engaging change agents.
There are 14 members in the team, and one evidence-based nursing expert is responsible for evidence-based training and project guidance; 1 Director of nursing department is responsible for project guidance; 1 orthopaedic medical specialist is responsible for clinical evidence application guidance; 1 Head nurse of the Nursing Department, responsible for coordinating the work; 2 head nurses in the ward were responsible for the application of evidence and supervision of the project process; Two nursing postgraduate students who have received systematic evidence-based nursing training are responsible for finding evidence, designing evidence application process, training team members on quality review methodology and process control, data summary and analysis, etc. Six key nurses in the ward acted as quality controllers, responsible for evidence implementation and data collection.
Phase 3: Context assessment and readiness for change.
Search GIN, NICE, SIGN, RNAO, NZGG, NIHR, NHS, and other guide networks, Cochrane, JBI, Campbell, and other systematic review databases according to the “6S” model. A total of 747 literature items were retrieved from EPIAP, WOCN, NZWCS, Wound Care Canada, and other professional associations. 703 literatures were removed after reading the title and abstract, and 11 literatures were included: 4 guidelines [8–11], 4 expert consensus [12–15], 2 systematic reviews [16,17], and 1 evidence summary [18]. The quality of the included guidelines was assessed using the AGREE II instrument; expert consensus and systematic reviews were appraised using the JBI critical appraisal tools; and the evidence summary was evaluated for its source rigor. This assessment was conducted independently by two researchers. FAME attributes were evaluated based on evidence: feasibility, suitability, clinical significance, and effectiveness. Members of the evidence-based project team were organized to sort out 39 best pieces of evidence... The final 36 pieces of evidence were categorized according to the SSKINS framework. Each review indicator was directly derived from and mapped to specific evidence recommendations, ensuring the intervention measures were grounded in the best available evidence. Evidence deemed not feasible or applicable to the local context (e.g., specific neck support types, waterproof plaster liners) was excluded after team discussion and consensus.
Baseline assessment and implementation:
Phase 4: Review of practice against evidence-based audit criteria.
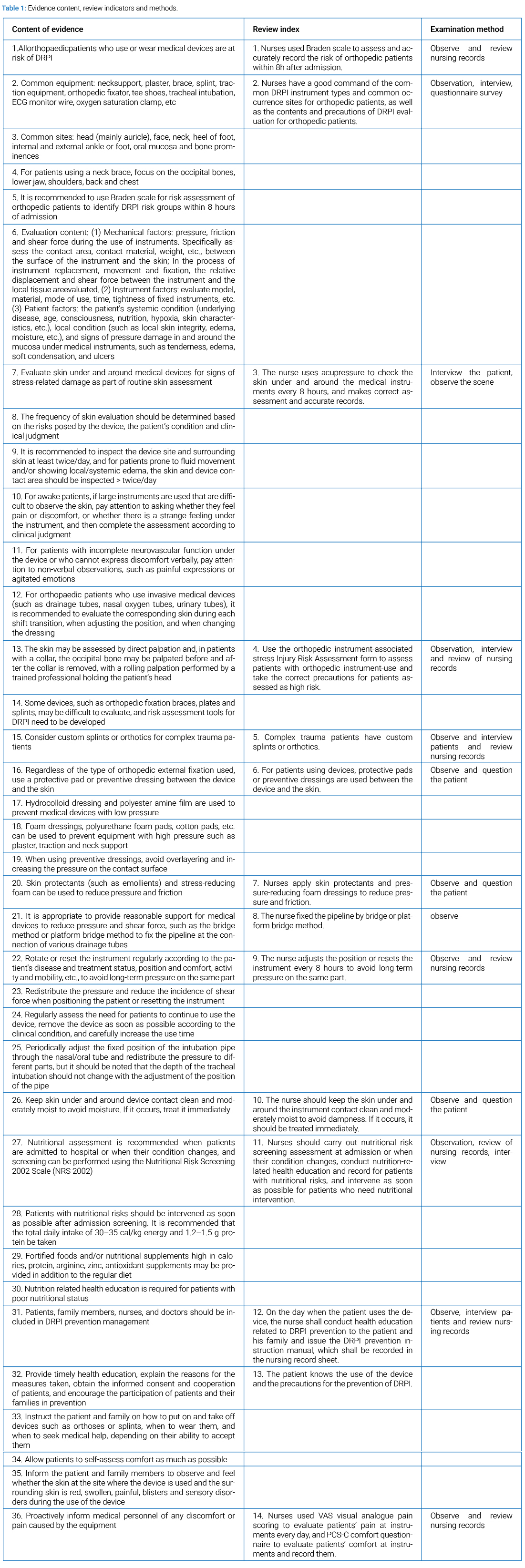
This study follows the Australian (Joanna Briggs Institute, JBI) clinical evidence application model, based on clinical practice. Use JBI’s online tool, Practice Application Of Clinical Evidence Systems (PACES), and Getting Research into Practice PACES (GRIP), to develop evidence-based practice protocols [19]. Regarding skin, the 12th evidence is monitoring the pressure effect on the skin. At present, no instrument has been introduced to measure the pressure on the skin, so it is excluded. In terms of support surface, Article 17: When a neck support is required for fixation, the appropriate type and material of the neck support should be selected, and the material of the neck support in our hospital is unified, so it is excluded; Article 29 Evidence should be added with a waterproof liner before using plaster, which should be removed because no waterproof plaster liner is available in the hospital at present. Finally, 36 pieces of evidence were included. To ensure the effective implementation of the 36 best pieces of evidence in clinical practice, 14 corresponding clinical review indicators were developed using the principle of similar combination. The contents, evaluation methods, and evidence sources of each indicator are shown in (Table 1).
Baseline review: This study selected the orthopedic ward of a first-class hospital in Wuhan as the research object, including 45 nurses who participated in evidence implementation, 61 orthopedic adult patients who received equipment fixation, and system resources related to the system process, environment, equipment, and other systems of the orthopedic ward. The department has 47 beds in total.
- A non-synchronous controlled experimental study was conducted, and a clinical quality review method was used to select adult orthopedic patients who received device fixation in a third-grade hospital in Wuhan as the study objects. The inclusion criteria were: 1) age ≥18 years old. 2) Use of medical devices for ≥ 8 hours. 3) Voluntary participation in this study. Finally, 61 patients were included, including 35 males and 26 females, aged 18–88 years, with an average age of 50 years.
- Nursing staff inclusion criteria: 1) Holding a nurse practitioner certificate. 2) Working in orthopedics for ≥ 1 year. 3) Voluntary participation in this study. Finally, 45 patients were included in the medical care, including 44 women and 1 man, aged 23–44 years old, with an average age of 29-year-old; 1–26 years of service, average 5 years; Title: 2 nurses, 21 nurses, 19 nurses in charge.
Obstacle factors and measures: From May to August 2024, the practice reform phase was completed with the support of Nursing Department leaders, chief physicians, and the Information Department. The evidence-based team conducted a discussion on obstacle factor analysis, listed indicators for a clinical compliance rate < 70%, analyzed obstacle factors using a brainstorming method one by one, and formulated the following action strategies, combined with the ward’s actual situation, to implement the evidence-based practice plan.
Obstacle factor 1: The compliance rate of indicator 4 was 0%. There is a lack of evaluation forms specifically used to evaluate orthopedic instrument-related stress injuries, and the department does not specify evaluation procedures for instrument-related stress injuries. Measures were formulated as follows: 1) Based on evidence summary and literature review analysis, combined with expert consensus, the “Orthopedic DRPI Risk Assessment Table” was constructed; 2) The “Orthopedic DRPI Assessment Process for Patients using Instruments” was constructed. Firstly, nurses conducted DRPI assessment, and the results were divided into low-risk (12 points), medium risk (12–18 points), and high risk (> 18 points), and corresponding measures were selected according to different risk levels; Secondly, the nurses instructed the patients to carry out self-assessment of comfort, and selected different measures according to the evaluation results. 3) The orthopedic DRPI should be included in the management of stress injuries, the quality control standards of stress injuries should be improved, and the specialized quality control items should be formed and included in the three-level quality control, which is specific to people. Including risk assessment (5 items), comfort assessment (2 items), stress reduction measures (5 items), skin protection measures (6 items), health education (4 items), stress injury supervision (8 items), stress injury training (2 items), and 32 items in 6 aspects.
Obstacle factor 2: The compliance rate of indicator 14 was 33.3%. The use and implementation of the patient self-comfort scale is insufficient. Measures are as follows: 1) Emphasize the importance of evaluating patients’ Comfort, and train nurses how to use the Chinese Version of the Perioperative Comfort Scale (PCS-C) to evaluate comfort. PCS consists of 18 items from 4 dimensions: physiological, psychological, sociocultural, and environmental, with each item scoring 1–4 points. 2) Patients’ subjective feelings of DRPI comfort were reflected through their self-reports.
Obstacle factor 3: The compliance rate of indicator 12 was 0%, and nurses lacked cognition. The measures are as follows: 1) Strengthen training, regularly organize nurses to summarize the common parts of orthopedics DRPI, formulate practice charts, explain the concept of DRPI, clinical manifestations, risk assessment, preventive measures, as well as the potential risks and coping strategies of different types of medical devices, the application principle and precautions of new dressings, etc. At the same time, personalized training can be conducted according to the educational background, professional title, work experience, and training needs of nurses, and basic knowledge training can be conducted for nurses with low seniority to help them master the basic concepts and preventive measures of DRPI. Advanced training for senior nurses to encourage them to learn and apply the latest research findings and best practices; Special training for wound therapists to improve their ability to recognize and manage DRPI. 2) Optimize workflow and establish DRPI prevention and management plan. Develop a complete DRPI prevention and management program based on evidence-based evidence and clinical experience, including risk assessment procedures and tools, medical device selection and use guidelines, preventive dressing selection and application guidelines, preventive skin care procedures, support surface and position change guidelines, nutritional support guidelines, education and verification procedures, etc. 3) The assessment is carried out by means of online questionnaire star survey and spot check.
Obstacle factor 4: The compliance rate of indicator 6 was 40.9%, and that of indicator 7 was 77%. Department lacks preventive products such as stress-relief stickers, hydrocolloids, etc. Measures are as follows: 1) The introduction of orthopedic stress injury prevention products. 2) Develop dressings with regenerative and repair functions. In view of the insufficient evidence of existing dressings, conduct original studies to explore the effects of new dressings, such as stem cell exosome dressings, and evaluate the biocompatibility, safety, effectiveness, and cost-effectiveness of new dressings.
Obstacle factor 5: The compliance rate of indicator 12 was 0%, the compliance rate of indicator 13 was 62.2%, and the health education on relevant preventive measures for patients and/or caregivers was not in place. The measures are as follows: 1) Improve patients’ participation and self-management ability. Organize DRPI health education training, produce and distribute DRPI Prevention Instruction Manual, and promote patients to master DRPI health knowledge through face-to-face education. 2) Emphasize patient participation, encourage patients to ask questions, and help patients better understand DRPI-related knowledge; Involve patients in decision-making, such as choosing appropriate precautions and developing a personal care plan. 3) Focus on high-risk groups, more detailed and frequent education for high-risk patients (e.g., identified via Braden score ≤16 or NRS 2002 ≥ 3), such as the elderly, malnourished, long-term bedridden patients, and provide more specific guidance, such as how to perform postures, how to choose and use preventive dressings. Personalized care plans were developed for these high-risk individuals.
Obstacle factor 6: The compliance rate of indicator 5 was 67.2%, and the medical device design was insufficient. Develop measures as follows: 1) Communicate with the manufacturer and provide suggestions to the manufacturer to improve the design, such as the use of softer and breathable materials, the addition of buffer layers, and the improvement of fixing methods. 2) Communicate with the doctor about the use of alternative products and ensure that their use will not affect the patient’s treatment. 3) Take protective measures: use protective pads, adjust the position, regularly check the part of medical equipment and skin contact, and timely detection and treatment of skin damage.
Obstacle factor 7: The compliance rate of indicator 5 was 67.2%, and the cooperation between nurses and doctors and instrument technicians was not close. The measures are as follows: 1) Strengthen communication and cooperation, and hold regular DRPI prevention and management meetings to discuss existing problems and establish improvement measures. 2) The DRPI reporting system encourages nurses to report DRPI in time. 3) Establish wound care teams, composed of experienced nurses and doctors, to guide the prevention and care of DRPI. 4) Communicate with the doctor in time to adjust the medical equipment.
Results
Baseline knowledge and attitude scores of nurses DRPI: The scores of nurses’ knowledge questionnaire ranged from 86 to 100 (88.31 ± 3.77) points, and the scores of APUP attitude questionnaire ranged from 28 to 40 (35.95 ± 3.30) points. Compared with 62–92 (78.31 ± 5.77) points of knowledge before training and 26–39 (31.86 ± 2.80) points of APUP attitude, the difference was statistically significant. (t = 5.867, P < 0.001)
Evidence application results:
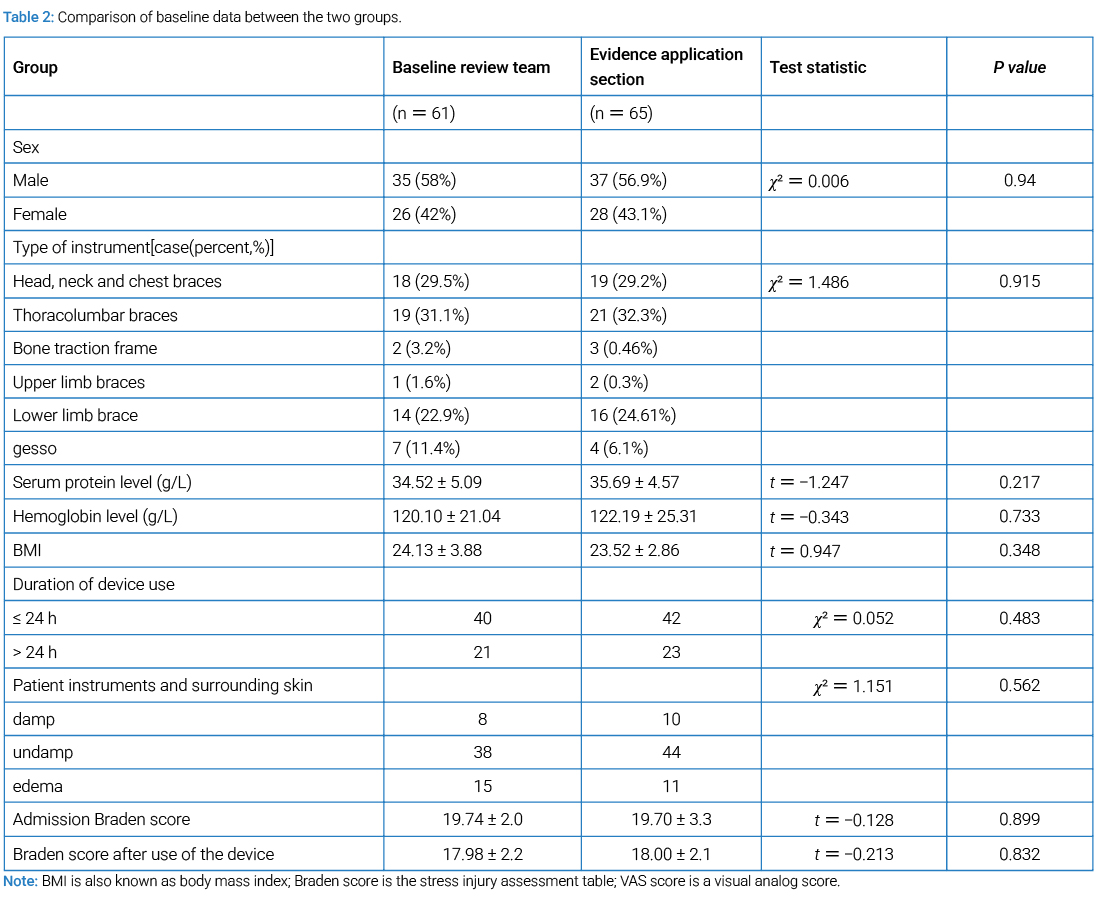
Comparison of general data of research objects: A total of 126 patients were included in this study, including 61 in the baseline review group and 65 in the evidence application group. There were no statistically significant differences between the two groups in device type, serum protein level, hemoglobin level, BMI, duration of device use, patient’s device and surrounding skin, Braden score after admission, and Braden score after device use (P > 0.05). The baseline was comparable, as shown in (Table 2).
Incidence of DRPI in 2 groups: The results of this study showed that the incidence of DRPI was 19.67% (12/61) in the baseline survey group and 3.07% (2/65) after the use of evidence.
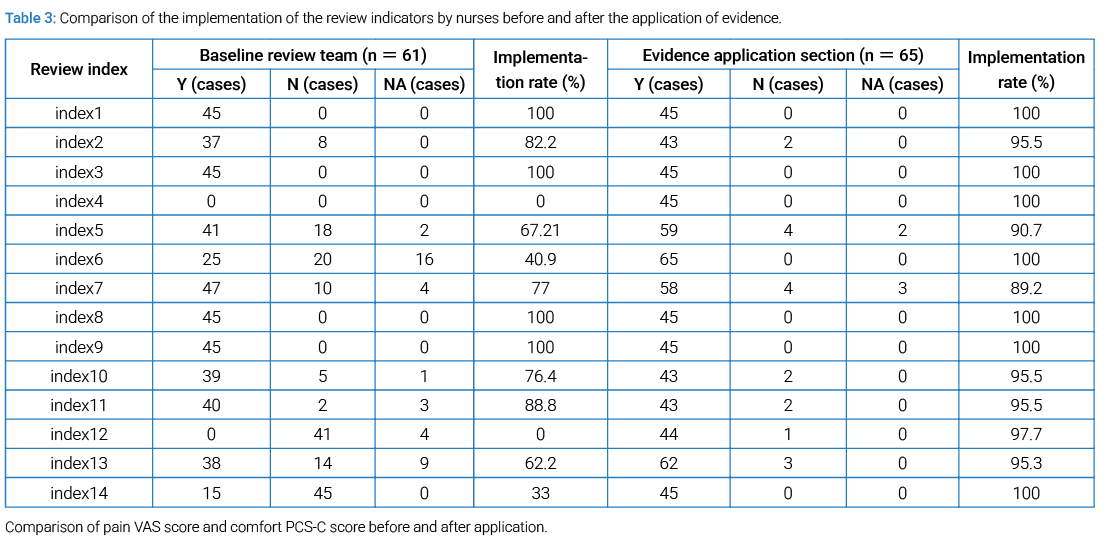
Clinical status review results of the best evidence for the prevention and management of orthopedic instrument-related stress injury: Before the application of evidence, the clinical implementation rate of 14 review indicators was 0–100%, among which the implementation rate of indicators 4, 5, 6, 12, 13, 14 & < 70%, after the application of evidence, the implementation rate of review indicators 1, 3, 4, 6, 8, 9, 14 was 100%; The implementation rate of indicator 4 using the “Orthopedic DRPI Risk Assessment Form” for risk assessment and indicator 12 conducting DRPI education to patients and issuing DRPI prevention guidance manual was increased from 0% to 100%; Indicator 5 patients with complex trauma used customized splints or orthotics, indicator 6 patients with instruments used protective pads or preventive dressings, indicator 13 patients knew the relevant contents of instruments, indicator 14 nurses used VAS and PCS-C to evaluate patient comfort every day, and the implementation rate of the review indicators was increased to more than 95%, as shown in (Table 3).
As can be seen from (Table 4), before and after the application of evidence, the VAS score of patients decreased from 2.0 points at baseline review time to 1.81 ± 0.39 points (P < 0.001). The PCS-C score of patients increased from 40.31 ± 3.85 at baseline to 44.82 ± 2.67 (P < 0.001). In addition, according to patients’ self-reports, patients’ self-reports that affect comfort also include: medical devices tend to cause skin moisture; Hopefully the cast will leave some space, because the elbow is sore; It is recommended that the size of the brace be enlarged appropriately to avoid the pressure caused by edema; In addition, it also mentioned the problems of itching inside the plaster and gypsum hardness; Finally, the patient reported that the mandibular part was inconvenient when eating, which was manifested as the buckle was not tight enough and was prone to shaking.

Discussion
The implementation of the evidence-based practice program has improved the clinical work: Patient diversity in terms of age, nutritional status, comorbidities, and type/duration of device use presents a challenge in DRPI prevention. Our strategy involved using standardized risk assessment tools (Braden, NRS 2002, Orthopedic DRPI Risk Assessment Form) to stratify patients and tailor the intensity and focus of interventions accordingly. For instance, nutritional support was prioritized for those at nutritional risk, and more frequent repositioning and skin checks were scheduled for patients with limited mobility or edema. This risk-stratified approach within the standardized SSKINS framework allowed for personalized care while maintaining protocol consistency, helping to mitigate potential outcome bias arising from patient heterogeneity. Studies [20] have shown that the more medical devices a patient uses, the higher the risk of a patient developing device-related stress injury. Orthopedic patients have a high risk of instrument-related stress injury due to their use of medical devices for a long time and prolonged home care, but there has been a lack of available risk assessment tables and management processes in clinical practice [21]. Therefore, based on the literature review and best evidence summary, combined with expert consensus, “Orthopedic Instrument-Related Stress Injury Risk Assessment Table” and “Orthopedic Instrument-Related Stress Injury Assessment Process” were constructed, and quality control indicators were formulated and incorporated into the management system. The incidence of DRPI in orthopedics decreased from 19.67% to 3.07% through the implementation of evidence-based programs. Knowledge scores of nurses increased from 62–92 (78.31 ± 5.77) to 86–100 (88.31 ± 3.77) (t = 5.867, P < 0.001). In addition, we used the PCS-C [22] questionnaire to evaluate the comfort of patients, and proposed corresponding measures according to the scores of different dimensions. The PCS-C score of patients increased from 40.31 ± 3.85 points at baseline review time to 44.82 ± 2.67 points (P < 0.001). The patients’ self-pain assessment showed that the VAS score decreased from 2.0 points at baseline review time to 1.81 ± 0.39 points (P < 0.001), so that the patient’s comfort state was improved.
The evidence-based practice promoted improvements in knowledge levels and changes in the behavioral norms of medical staff to prevent DRPI: Medical personnel are aware of evidence and recognize evidence as the basis for applying nursing evidence to clinical practice. Medical personnel are the practitioners and coordinators of applying evidence-based evidence to clinical practice, so it is necessary to increase the training of relevant knowledge and clinical skills for medical personnel [23]. The best evidence-based practice measures adopted in this study significantly improved nurses’ knowledge of DRPI. A number of indicators were examined by means of a questionnaire, including scores on basic knowledge and attitude questionnaires. The results of the survey showed that the scores of nurses in DRPI basic knowledge ranged from 62 to 92 points (average 78.31 ± 5.77 points), and the overall level was low, which indicated that nurses’ grasp of DRPI-related knowledge was insufficient, and systematic training and learning were urgently needed. In addition, APUP attitude questionnaire scores ranged from 28 to 40 points (mean 35.95 ± 3.30 points), which also indicated room for improvement. In terms of specific indicators, for example, the compliance rate of skin protectant or stress relief patches shown in indicator 7 is 77%, indicating that in orthopedic DRPI prevention management, nurses have a relatively low compliance rate when using these protective measures, and the skin condition under medical equipment is not receiving enough attention. In addition to the impact of insufficient preventive dressing prepared by the department, it also reflects that the lack of nurses’ own knowledge restricts the effective development of clinical practice. These findings highlight the importance of systematic training, covering all aspects from theoretical instruction to practice, from risk assessment to health education, aimed at facilitating the successful translation of best evidence into clinical practice. In view of the wide variety of orthopedic medical equipment, in order to facilitate management and improve efficiency, medical personnel worked together to develop a “orthopedic common equipment classification and prevention site tips table.” This initiative will not only help standardize clinical procedures but also improve the implementation rate of preventive measures. Through the implementation of the evidence-based practice program, the knowledge and behavior of health care workers in the prevention of DRPI have been improved, and initial results have been achieved.
Strengthening the communication and multidisciplinary cooperation of medical technology team members is an important guarantee for evidence-based practice: Strengthening communication and multidisciplinary cooperation among members of the medical technology team is an important guarantee for evidence-based practice. In the course of evidence-based practice, we noticed that patients often faced skin compression, moisture, and low comfort due to limitations in device material and design. In addition, the weight of the medical device itself may also cause muscle soreness in the patient, which in turn reduces the patient’s time and willingness to move, and ultimately increases the incidence of DRPI. Therefore, there is an urgent need for the participation of nurses, doctors, and technicians to form an effective collaborative mechanism. As front-line nurses, nurses should timely and accurately assess patients’ conditions, and promptly feedback relevant information to doctors and technicians, so that the three parties can participate in the improvement process of medical equipment and promote the conversion and application of the latest evidence in clinical practice.
Cite this article
Xu R, Chen K. The optimal evidence application for the mitigation of pressure damage associated with orthopedic instruments: Rooted in SSKINS cluster management. Clin Surg J. 2026;7(1):1–10.
