Abstract
Lymphoepithelial Cyst arising from the submandibular gland is a rare finding. In this article, we propose to highlight the inclusion of LEC in the differential diagnosis of neck swellings.
We present a case of a 20-year-old male patient who presented to our ENT department with complaints of a swelling in the right submandibular region for 2 months. On examination, a well-demarcated swelling approximately 3 cm × 3.5 cm in size was found involving the right submandibular triangle. Mass was mobile, firm to cystic in consistency, and non-tender. The overlying skin was normal, and the swelling was non-fluctuant. No other palpable lymph nodes on neck examination were found clinically.
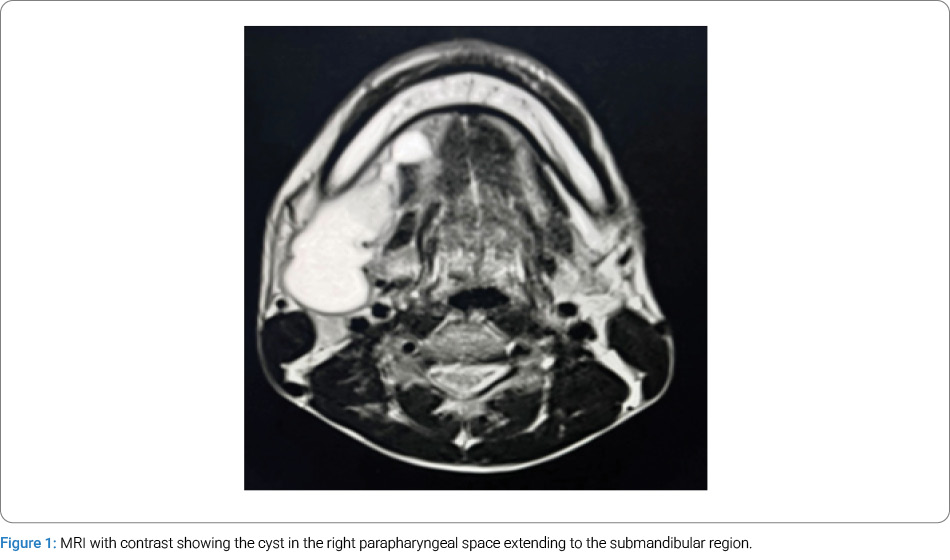
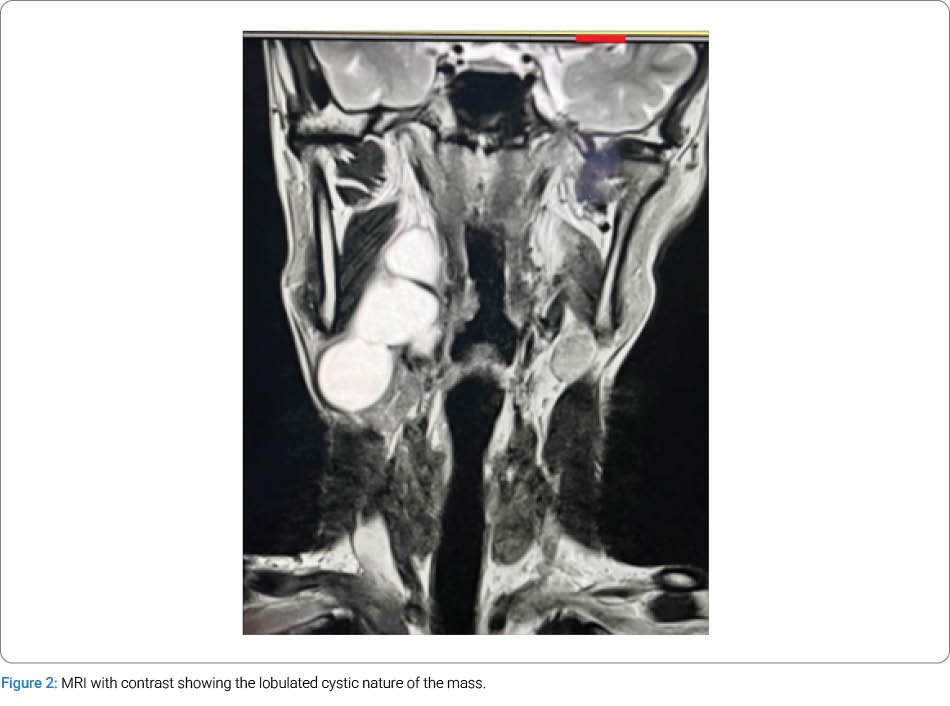
On intraoral examination, pushing of the right tonsil medially causes minimal narrowing of the oropharynx. MRI of the neck showed a thick-walled cystic lesion in relation to the right parapharyngeal space with extension to the submandibular region. The case was posted for surgical excision under general anesthesia, wherein the superficial part of the right submandibular gland was found deeply attached to the cyst and was partially excised along with the cyst. Histopathology suggested a Lymphoepithelial Cyst undergoing hemorrhage and inflammation.
A rare case of neck swelling in the submandibular region can include a Lymphoepithelial Cyst in the differential diagnosis.
Abbreviations
LEC: Lymphoepithelial Cyst
MRI: Magnetic Resonance Imaging
FNAC: Fine Needle Aspiration Cytology
CT Scan: Computed Tomography Scan
Introduction
Lymphoepithelial cysts (LECs) are benign, slow-growing lesions that may be unilocular or multilocular in the head and neck region. Among the salivary glands, the parotid gland is more commonly affected, while it is rarer in the submandibular gland. They can also occur in the floor of the mouth. They usually cause no pain but may be associated with discomfort over the affected region, a feeling of a lump in the throat, and concerns of cosmetic deformity. If not promptly and appropriately treated, they have a propensity for malignant transformation. Review of literature failed to show any definitive classification of LEC. One such case of a rare Lymphoepithelial Cyst (LEC) arising from the right superficial part of the submandibular gland with extension to the right parapharyngeal space in a 20-year-old patient is presented herewith because of the rarity, with a review of the literature.
Case Presentation
Mr. V. H. a 20-year-old male patient, reported to our ENT clinic on August 27, 2024, with complaints of right-sided neck swelling of 2 months duration. The swelling was gradually increasing in size. Initially, there was no pain, but gradually developed a sensation of a lump in the throat and mild difficulty in swallowing. The patient was not a known diabetic nor a hypertensive. There was no history of any food or drug allergy. On clinical examination, a well-demarcated swelling of approximately 3 cm × 3.5 cm in size involving the right submandibular triangle was found. Mass was mobile, firm to cystic in consistency, and non-tender. Oral cavity examination showed pushing of the right tonsil medially, causing minimal narrowing of the oropharynx. An Magnetic resonance imaging (MRI) of the Neck with contrast was done on August 27, 2024, which showed a thick-walled cystic lesion in relation to the right parapharyngeal space with extension to the submandibular region. The lesion was thick-walled and lobulated. A T2 hyperintense cystic lesion measuring 72 mm × 50 mm × 20 mm was seen in relation to the right lateral oropharyngeal wall with further extension along the anterior aspect of the right carotid sheath into the medial aspect of the angle of mandible and the ipsilateral submandibular region (Figure 1, Figure 2). There is mild post-contrast enhancement of the cyst wall without a solid enhancing nodule. Imaging findings raised the possibility of Second branchial cleft cyst. Fine Needle Aspiration Cytology (FNAC) was suggested, but the patient was reluctant to undergo it as it had been tried earlier elsewhere with inconclusive results. Hematological and biological investigations were found to be within normal limits.
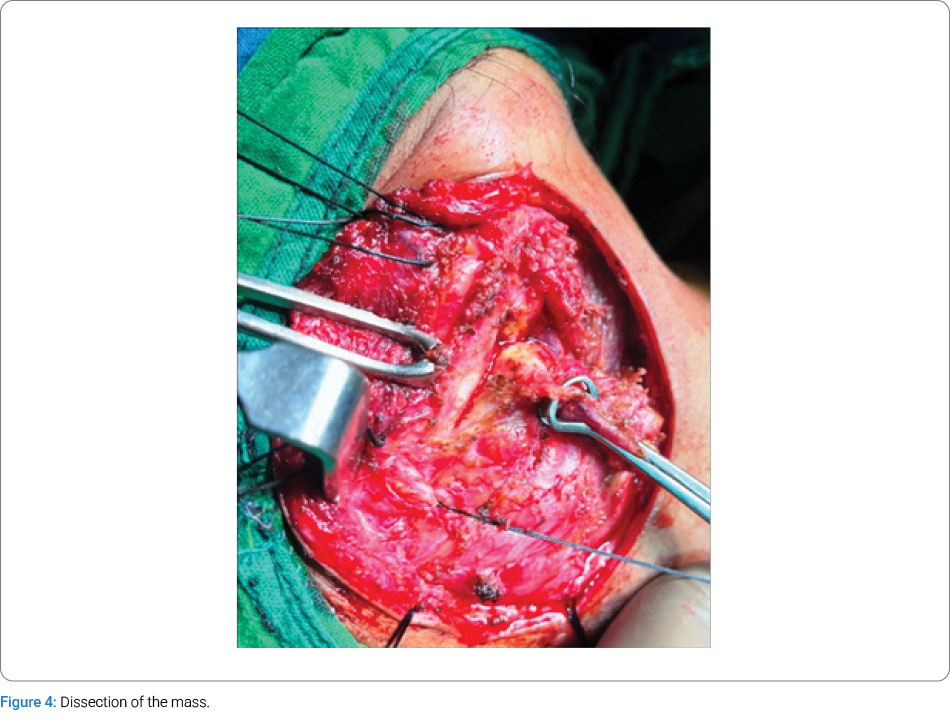
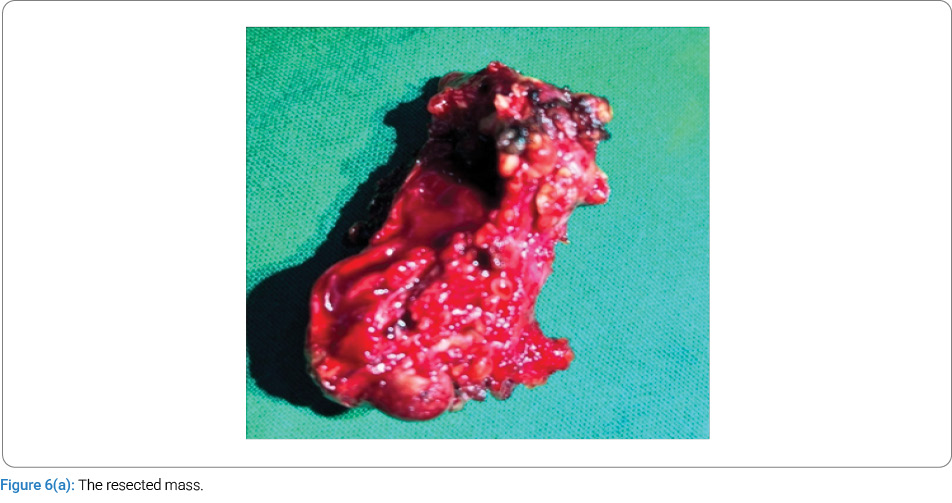
The patient was posted for surgical excision of the mass on August 30, 2024 under general anesthesia. The patient was positioned with right-sided neck extension. 2% Xylocaine with adrenaline infiltrated was in the incision line. Curved neck incision was given 2 fingers’ breadth below the lower border of the right mandible (Figure 3). Subplatysmal dissection was carried out with pencil diathermy and bipolar cautery. A large cystic mass was seen engulfing the right submandibular gland with the extension to the right pre-styloid parapharyngeal space (Figure 4, Figure 5). The right common facial vein and right facial artery were ligated and divided. The cystic lesion was carefully cleared from the deep lobe of the submandibular gland. However superficial part of the gland was found deeply attached to the cyst and had to be partially excised along with the cyst. The whole cyst was mobilized carefully from the prestyloid compartment of the right parapharyngeal space and excised (Figure 6a, Figure 6b). Hemostasis was achieved, and the wound was closed in two layers. The histopathology report showed a picture of a cystic lesion with hemorrhage lined by attenuated epithelium (mostly cuboidal). The wall was composed of unremarkable salivary gland tissue, reactive lymphoid tissue including prominent germinal centers, and polymorphic inflammatory infiltrate including hemosiderin laden macrophages and fibroblast. Fibrofatty and muscle tissue are also noted on the extreme outer surface. The overall picture was suggestive of a LEC undergoing hemorrhage and inflammation. No other abnormality was seen. The case was reviewed on May 30, 2025, showed no clinical evidence of recurrence of the cyst, and the patient was pleased with the outcome of the surgery. However, there is a hypertrophied scar on the incision line (Figure 7), which can be managed by a plastic surgery procedure at a later date if the patient is concerned. The patient is scheduled for routine follow-up.



Discussion
LECs are rare in the neck and are more rarely seen arising from the submandibular salivary gland, engulfing the whole gland, or arising from the superficial lobe of the gland. These are slow-growing cysts that can be unilocular or multilocular. In certain cases, it has been reported that such swellings can have a rapid increase in size, leading to difficulty in mastication Iqbal et al. [1]. They are also called branchial cysts and commonly arise from the parotid gland and the oral cavity, and are often found in adults. Hazarika et al. [2] reported a case of mucocele of the submandibular gland, also a cystic lesion mimicking a deep plunging ranula. Occasionally, LEC was also seen in the neck without involving the salivary gland, located in the anterior triangle of the neck, and is commonly seen in children. LEC sizes may vary from 0.5 cm to more than 5 cm. An expanding cyst may involve the neck spaces, including the parapharyngeal space, producing various pressure symptoms like a feeling of a lump in the neck, difficulty in swallowing, as seen in our case. Ahmed et al. [3] stated that these cysts, if not treated, have a high chance of transforming into malignant lesions such as malignant lymphomas, which have the capacity to involve the extranodal sites secondarily.
LECs are slow-growing lesions commonly seen in females in their second or third decade of life in 60%–80% of cases. The LECs are usually associated with the salivary gland, especially the parotid gland, and very rarely with the submandibular salivary gland Ioachim [4]. Most cases of the LEC of the salivary gland have an attachment to the superficial surface of the submandibular gland, but rarely the gland and duct may also be affected Tiwari et al. [5]. The branchial cyst, which does not involve the salivary gland, usually arises on the lateral cervical area, classically described to occur anterior to the upper third of the sternocleidomastoid muscle.
Etiologically, LEC may be of congenital origin, or it may be due to the lymph node theory. It is proposed that cysts developed due to cystic transformation of the lymph node. LEC can arise with other conditions like Sjogren’s syndrome, Mikulicz disease, and myoepithelial sialadenitis Panchbhai et al. [6]. Lymphoepithelial cyst has also been associated with Human Immunodeficiency Virus (HIV) infection as a part of a diffuse infiltrative lymphocytosis syndrome. It is usually bilateral and is accompanied by cervical lymphadenopathy Rojas et al. [7].
Investigation modalities include ultrasound neck, FNAC, CT scan, and MRI of the neck with contrast. MRI of the neck with contrast is found to be more accurate in knowing the extension of the cyst, as has been seen in our case.
The lesions of salivary glands with a prominent lymphoid component are a heterogeneous group of diseases that include benign reactive lesions and malignant neoplasms. The differential diagnosis includes lymphoepithelial sialadenitis, HIV associated salivary gland disease, chronic sclerosing sialadenitis, Warthin tumor, extranodal marginal zone B-cell lymphoma, salivary duct retention cyst (mucocele), dysgenetic polycystic disease of the salivary gland, and mucosa-associated lymphoid tissue lymphoma. Patients with salivary gland LECs are at an increased risk of developing lymphoma; hence, they should be treated early with excision of the cyst. Complete excision of the cyst with partial excision of the attached salivary gland should be ideal to prevent recurrence Habib et al. [8] than only simple excision of the cyst. Routine follow-ups are necessary to check for any recurrence, especially in the early years.
Cite this article
Hazarika P, Baruah A, Sarma N, Deka T. Lymphoepithelial cyst of right submandibular gland: a rare clinical entity with review of literature. Clin Surg J. 2026;7(1):1–4.
Keywords
Lymphoepithelial cyst; Branchial cyst; Parapharyngeal space; Submandibular gland
Copyright
© 2026 Produl Hazarika. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
