The Role of Neoadjuvant Treatment in HER-2 Positive Breast Cancer: What a Surgeon Should Know
* Pasquale Auricchio;
Christoph Mayr;
Romano Polato;
Antonio Frena;
-
* Pasquale Auricchio: Department of General Surgery–Breast Unit, EUSOMA Center, Azienda Sanitaria dell’Alto Adige, Bolzano, Italy
-
Christoph Mayr: Department of General Surgery–Breast Unit, EUSOMA Center, Azienda Sanitaria dell’Alto Adige, Bolzano, Italy
-
Romano Polato: Department of General Surgery–Breast Unit, EUSOMA Center, Azienda Sanitaria dell’Alto Adige, Bolzano, Italy
-
Antonio Frena: Department of General Surgery, Azienda Sanitaria dell’Alto Adige, Bolzano, Italy
Abstract
This review aims to provide an updated overview of neoadjuvant strategies in Human Epidermal Growth Factor Receptor 2 (HER2)-positive breast cancer, with a specific focus on surgical implications. We explore the role of targeted therapies, critical trial data, and future treatment directions. Particular attention is given to the impact of Neoadjuvant Therapy (NAT) on surgical outcomes such as Breast-Conserving Surgery (BCS) rates, axillary management, and reoperation risk. By offering a critical synthesis of current evidence, this review intends to support breast surgeons in understanding and applying neoadjuvant protocols in clinical practice.
Abbreviations
HER2: Human Epidermal Growth Factor Receptor 2; NAT: Neoadjuvant Therapy; pCR: Pathologic Complete Response; BCS: Breast-Conserving Surgery; ALND: Axillary Lymph Node Dissection; TAD: Targeted Axillary Dissection; HR: Hormone Receptor; T-DM1: Trastuzumab Emtansine; T-DXd: Trastuzumab Deruxtecan; ADC: Antibody-Drug Conjugate; TKI: Tyrosine Kinase Inhibitor; CNS: Central Nervous System; TILs: Tumor-Infiltrating Lymphocytes; PET: Positron Emission Tomography; ESMO: European Society for Medical Oncology; NCCN: National Comprehensive Cancer Network; EGFR: Epidermal Growth Factor Receptor
Introduction
Human Epidermal Growth Factor Receptor 2 (HER2)-positive breast cancer, representing 15%–30% of all breast cancers, is characterized by the overexpression of the HER2 receptor and is associated with aggressive clinical behavior and poor prognosis [1,2]. The introduction of targeted therapies, such as trastuzumab and pertuzumab, has revolutionized treatment and significantly improved survival [3,4]. Despite these advances, treatment resistance and recurrence remain significant challenges [5,6], underscoring the need for multimodal approaches, such as Neoadjuvant Therapy (NAT) [7–21].
Methods
This review employed a narrative approach. A comprehensive literature search was performed in PubMed, Scopus, and Web of Science databases from January 2010 to March 2025. The following search terms were used individually and in combination: “HER2-positive breast cancer”, “Trastuzumab”, “Pertuzumab”, “Antibody-Drug Conjugate (ADC)”, “surgical outcomes”, “Pathologic Complete Response (pCR)”, and “axillary management”. The inclusion criteria encompassed clinical trials, meta-analyses, guidelines, and high-quality narrative reviews published in the English language. Exclusion criteria included preclinical studies, single case reports, non-peer-reviewed articles, and publications without clear relevance to neoadjuvant HER2-positive breast cancer.
The final selection included 63 peer-reviewed articles. Priority was given to large randomized controlled trials, landmark studies, and publications from high-impact journals. The selection process involved independent screening of titles and abstracts by two authors, with discrepancies resolved through discussion.
Clinical Efficacy of Neoadjuvant Therapy
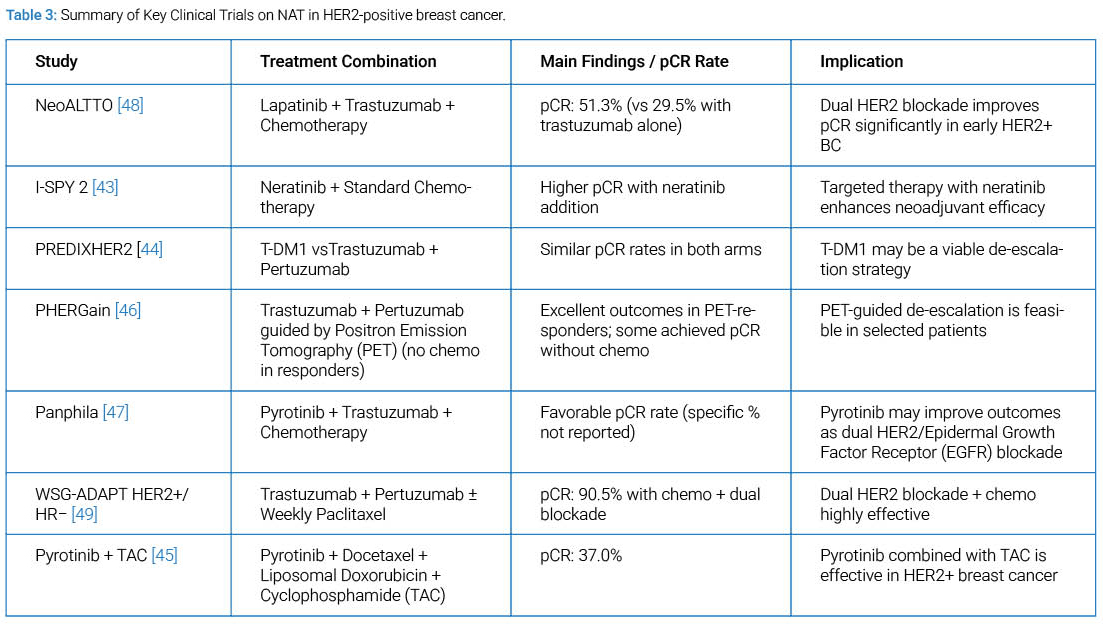
Pathologic Complete Response (pCR): Achieving a pCR, defined as the absence of invasive cancer in breast and axillary nodes post-therapy, is a surrogate marker for improved disease-free and overall survival in HER2+ patients [22,23]. Studies such as CTNeoBC and NeoALTTO confirm that dual HER2 blockade with trastuzumab and pertuzumab significantly increases pCR rates (up to 60%) [24–28,48]. pCR is highest in Hormone Receptor (HR)-negative/HER2+ subtypes.
Impact on Survival: Meta-analyses show strong correlations between pCR and long-term outcomes. For HER2+ patients, those achieving pCR exhibit up to 70%–80% improvement in event-free and overall survival compared to those with residual disease [29,30].
Surgical Implications
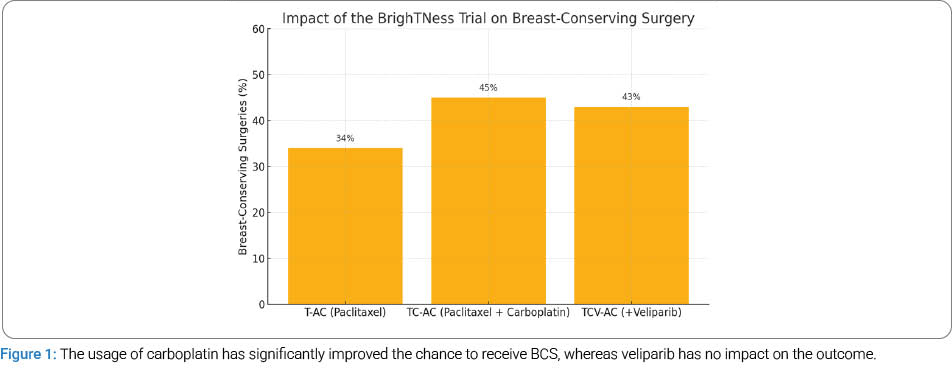
Conversion to Breast-Conserving Surgery (BCS): NAT often enables conversion from mastectomy to lumpectomy. Trials like BrighTNess (Figure 1) for triple negative breast cancer reported significant increases in BCS eligibility following NAT, which is also confirmed specifically in the TECHNO trial for HER2-positive (Figure 2). Tumor shrinkage also facilitates better cosmetic outcomes and fewer reoperations [31,32].
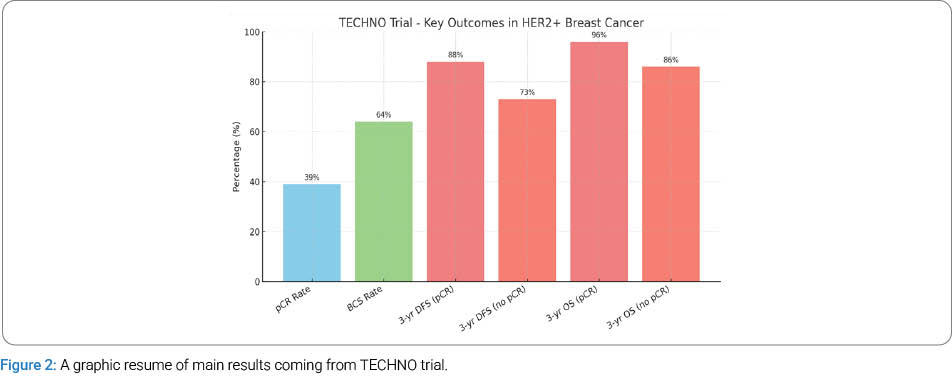
Margin Status and Reoperation Rates: NAT improves the likelihood of achieving negative margins at the time of initial surgery, thereby reducing the risk of re-excision. This effect is particularly evident in patients undergoing BCS, where margin status is a critical determinant of success. For instance, the First Surgical National Consensus Conference of the Italian Breast Surgeons Association (ANISC) highlighted that NAT significantly enhances the rate of margin-negative resections in HER2-positive breast cancer, enabling more effective surgical planning and reducing reoperation rates [33]. Furthermore, findings from the TECHNO trial and other large-scale datasets suggest that patients treated with NAT have fewer margin-positive resections and improved cosmetic outcomes, supporting a more conservative surgical approach [32].
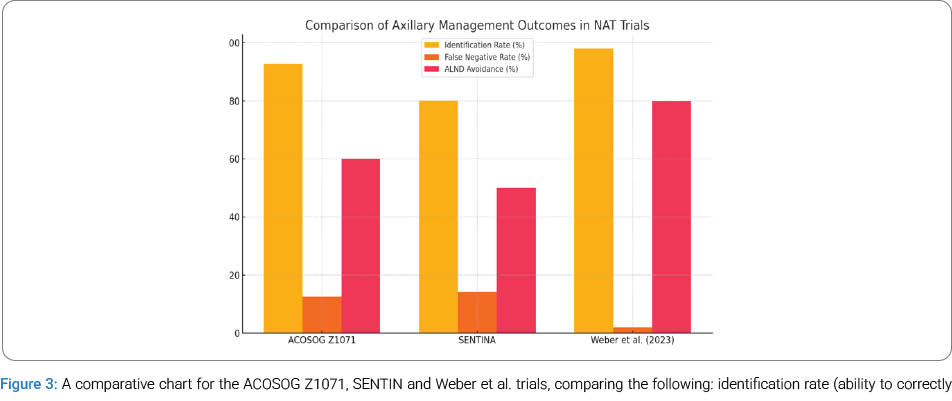
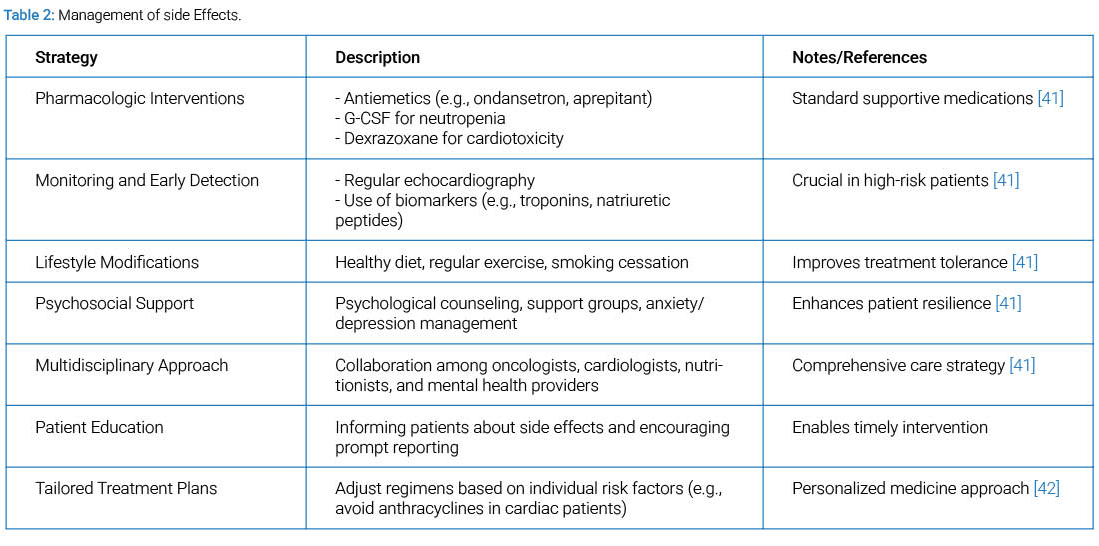
Axillary Management: NAT can significantly downstage axillary lymph node disease, converting Clinical Node-Positive Disease (cN1) to Pathological Node-Negative Disease After Neoadjuvant Therapy (ypN0) status. This response enables a shift from ALND to less invasive techniques such as Sentinel Lymph Node Biopsy (SLNB) or TAD [33]. TAD, which involves the removal of both sentinel and pre-marked positive nodes, has demonstrated high identification rates and a low false-negative rate in patients treated with NAT. This approach has been endorsed by trials such as ACOSOG Z1071, SENTINA, and, more recently, by Weber et al. [34], who showed that omitting ALND in select patients post-NAT does not compromise oncologic outcomes but significantly reduces surgical morbidity, such as lymphedema, seroma, and shoulder dysfunction [35–37]. These findings support a tailored surgical approach to the axilla based on treatment response (Figure 3) (Table 1,Table 2).
Combination Therapies and Emerging Agents
Dual HER2 Blockade: Dual HER2 blockade with trastuzumab and pertuzumab is considered the gold standard in NAT for HER2-positive breast cancer [19]. The NeoALTTO trial [48] demonstrated significantly higher pCR rates when trastuzumab was combined with lapatinib or pertuzumab compared to trastuzumab alone. The CTNeoBC pooled analysis [28] confirmed that dual blockade achieves the most pronounced survival benefit in HR-negative subgroups. For patients with residual disease post-NAT, the KATHERINE trial [44] established the superiority of Trastuzumab Emtansine (T-DM1) over trastuzumab alone, reducing the risk of invasive disease recurrence by 50%.
Novel Agents: Among the most promising emerging therapies, Trastuzumab Deruxtecan (T-DXd), an ADC, has shown remarkable efficacy in heavily pretreated HER2-positive metastatic patients, including those with brain metastases, as demonstrated in DESTINY-Breast03 [50,54,56]. Likewise, margetuximab, an Fc-optimized anti-HER2 antibody, offers improved Antibody-Dependent Cellular Cytotoxicity (ADCC) over trastuzumab [50]. In addition, tucatinib, a HER2-selective Tyrosine Kinase Inhibitor (TKI), has demonstrated Central Nervous System (CNS) activity in the HER2CLIMB trial, making it an important option for patients with brain involvement [51]. Furthermore, pyrotinib, a pan-HER TKI, is under evaluation in multiple Asian trials with encouraging results in terms of response rate and pCR in the neoadjuvant setting [45].
Immunotherapy: Immunotherapy is an emerging frontier in HER2-positive breast cancer. Preliminary studies suggest that combining HER2-targeted therapies with immune checkpoint inhibitors such as atezolizumab or pembrolizumab may enhance immune response, particularly in tumors with high levels of Tumor-Infiltrating Lymphocytes (TILs). Early-phase trials, including the PANACEA study [52], have reported encouraging responses in HER2-enriched subtypes. The integration of immunotherapy into the neoadjuvant setting may expand treatment options for patients with poor responses to standard regimens, although further randomized data are required to establish efficacy (Table 3).
Current Guidelines and Recommendations
ESMO and NCCN recommend neoadjuvant systemic therapy with dual HER2 blockade—trastuzumab and pertuzumab—combined with taxane-based chemotherapy as the standard for patients with stage II–III HER2-positive breast cancer [10,16,50]. This regimen has demonstrated high pCR rates and improved long-term survival outcomes, particularly in HR-negative tumors.
For patients who achieve pCR after NAT, current guidelines support continuation of anti-HER2 therapy to complete one full year of treatment. This often consists of trastuzumab alone or in combination with pertuzumab, depending on nodal status and initial disease burden [50,51].
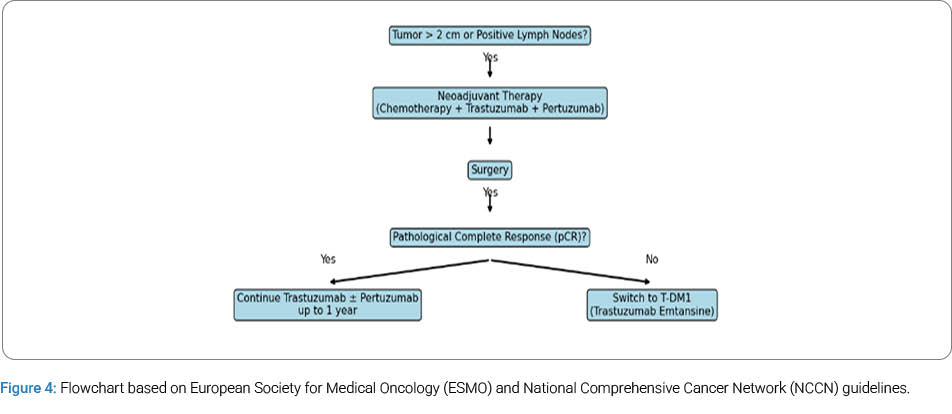
In cases where pCR is not achieved, adjuvant treatment with T-DM1 is strongly recommended, as demonstrated by the KATHERINE trial, which showed superior invasive disease-free survival compared to continued trastuzumab in patients with residual disease (Figure 4). De-escalation strategies are being actively explored in clinical trials, notably PHERGain and WSG-ADAPT HER2+/HR− [53]. These studies are investigating whether selected patients—identified through early response imaging or biomarkers—can safely avoid chemotherapy altogether and be treated effectively with anti-HER2 agents alone or with minimal systemic toxicity. Interim results suggest promising pCR rates and low recurrence risk in low-burden, high-response subsets [54–56].
Discussion
NAT not only improves oncologic control but also significantly enhances surgical management in HER2-positive breast cancer [57–59]. Evidence from trials such as TECHNO and BrighTNess demonstrates increased eligibility for BCS following tumor shrinkage, with rates increasing from below 50% to over 70% post-NAT. Moreover, the ANISC consensus and data from Untch et al. [32] confirm that NAT leads to higher rates of margin-negative resections, reducing the need for reoperations.
In addition to these advances in breast surgical management, the ability of NAT to downstage axillary disease has been transformative. The ACOSOG Z1071 and SENTINA trials established the foundation for replacing full Axillary Lymph Node Dissection (ALND) with Targeted Axillary Dissection (TAD), minimizing morbidity without compromising oncologic safety. More recently, Weber et al. [34] validated this strategy in a large contemporary cohort, confirming its role in tailored surgical de-escalation.
At the systemic level, dual HER2 blockade with trastuzumab and pertuzumab remains a cornerstone, supported by data from NeoALTTO and CTNeoBC, which demonstrate elevated pCR rates, particularly in HR-negative tumors. For patients with residual disease, the KATHERINE trial showed that adjuvant T-DM1 significantly improves invasive disease-free survival compared to trastuzumab alone [60].
The emergence of novel anti-HER2 agents, such as T-DXd margetuximab, tucatinib, and pyrotinib, introduces opportunities to overcome resistance to first-line therapies and address metastases, including those in the CNS. Immunotherapy combinations, particularly those involving checkpoint inhibitors like atezolizumab, are also under active investigation and may shape the future of treatment for HER2-enriched subtypes.
Despite these advancements, a major unmet need persists in the identification of robust biomarkers to guide treatment stratification. Trials such as PHERGain and WSG-ADAPT HER2+/HR− are pioneering de-escalation strategies guided by early imaging (e.g., 18F-FDG-PET) and TILs. These approaches aim to individualize therapy, potentially sparing selected patients from the toxicity of chemotherapy while preserving efficacy.
In summary, NAT in HER2-positive breast cancer has evolved from a purely oncologic intervention into a multidimensional strategy that optimizes surgical outcomes, improves survival, and paves the way for precision oncology through de-escalation and emerging targeted modalities.
Conclusion
NAT is transformative in HER2+ breast cancer, significantly impacting survival and surgical outcomes. Surgeons must understand its implications on margin status, axillary approach, and reoperation risk. Future directions include individualized therapy guided by response and molecular profiling, with growing roles for novel anti-HER2 agents and immunotherapy.
Simple Summary
NAT improves surgical outcomes for HER2-positive breast cancer by reducing tumor size and lymph node involvement, thereby increasing eligibility for BCS and decreasing the need for axillary dissection. This enhances margin clearance, lowers local recurrence rates, and provides early information about tumor biology and treatment responsiveness, which is critical for surgical planning.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lv Q, Meng Z, Yu Y, Jiang F, Guan D, Liang C, et al. Molecular mechanisms and translational therapies for human epidermal receptor 2 positive breast cancer. Int J Mol Sci. 2016;17(12):2095.
- Krishnamurti U, Silverman JF. HER2 in breast cancer: A review and update. HER2 in Breast Cancer: A Review and Update. Adv Anat Pathol. 2014;21(2):100–107.
- Vu T, Sliwkowski MX, Claret FX. Personalized drug combinations to overcome trastuzumab resistance in HER2-positive breast cancer. Biochim Biophys Acta. 2014;1846(2):353–365.
- Geurts SME, Ibragimova KIE, Ding N, Meegdes M, Erdkamp F, Heijns JB, et al. Time trends in real-world treatment patterns and survival in patients diagnosed with de novo HER2+ metastatic breast cancer: an analysis of the SONABRE registry. Breast Cancer Res Treat. 2024;205(2):287–302.
- Garrido-Castro AC, Regan MM, Niman SM, Nakhlis F, Remolano C, Rosenbluth JM, et al. Clinical outcomes of de novo metastatic HER2-positive inflammatory breast cancer. NPJ Breast Cancer. 2023;9(1):50.
- Wahler J, Suh N. Targeting HER2-positive breast cancer with chemopreventive agents. Curr Pharmacol Rep. 2015;1(5):324–335.
- Biganzoli L, Battisti NML, Wildiers H, McCartney A, Colloca G, Kunkler IH, et al. Updated recommendations regarding the management of older patients with breast cancer: a joint paper from the European Society of Breast Cancer Specialists (EUSOMA) and the International Society of Geriatric Oncology (SIOG). Lancet Oncol. 2021;22(7):e327–e340.
- Burstein HJ, Curigliano G, Thürlimann B, Weber WP, Poortmans P, Regan MM, et al. Customizing local and systemic therapies for women with early breast cancer: the St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann Oncol. 2021;32(10):1216–1235.
- Carrión-García PY, Sánchez-Domínguez CN, Gallardo-Blanco HL, Garza-Treviño EN, Delgado-Balderas JR, Roacho-Pérez JA, et al. Aptamer-conjugated gold nanoparticles targeting human epidermal growth factor receptor 2 (HER2) for cancer theranostic. In vitro assays. Materials Proceedings. 2023;14(1):25.
- Curigliano G, Burstein HJ, Gnant M, Loibl S, Cameron D, Regan MM, et al. Understanding breast cancer complexity to improve patient outcomes: the St Gallen International Consensus Conference for the Primary Therapy of Individuals with Early Breast Cancer 2023. Ann Oncol. 2023;34(11):970–986.
- Freedman RA, Minami CA, Winer EP, Morrow M, Smith AK, Walter LC, et al. Individualizing surveillance mammography for older patients after treatment for early-stage breast cancer: multidisciplinary expert panel and International Society of Geriatric Oncology consensus statement. JAMA Oncol. 2021;7(4):609–615.
- Nakashoji A, Hayashida T, Yokoe T, Maeda H, Toyota T, Kikuchi M, et al. The updated network meta-analysis of neoadjuvant therapy for HER2-positive breast cancer. Cancer Treat Rev. 2018:62:9–17.
- Triantafyllidi E, Triantafillidis JK. Systematic review on the use of biosimilars of trastuzumab in HER2+ breast cancer.Biomedicines. 2022;10(8):2045.
- Gupta GK, Collier AL, Lee D, Hoefer RA, Zheleva V, van Reesema LLS, et al. Perspectives on triple-negative breast cancer: Current treatment strategies, unmet needs, and potential targets for future therapies. Cancers (Basel). 2020;12(9):2392.
- Ménard S, Fortis, S, Castiglioni F, Agresti R, Balsari A. HER2 as a prognostic factor in breast cancer. Oncology. 2001:61 Suppl 2:67–72.
- Kaidar-Person O, Dahn HM, Nichol AM, Boersma LJ, de Ruysscher D, Meattini I, et al. A Delphi study and International Consensus Recommendations: The use of bolus in the setting of postmastectomy radiation therapy for early breast cancer. Radiother Oncol. 2021:164:115–121.
- Lambertini M, Ferreira AR, di Meglio A, Poggio F, Puglisi F, Sottotetti F, et al. Patterns of care and clinical outcomes of HER2-positive metastatic breast cancer patients with newly diagnosed stage IV or recurrent disease undergoing first-line trastuzumab-based therapy: a multicenter retrospective cohort study. Clin Breast Cancer. 2017;17(8):601–610.e2.
- Pluta P, Jesionek-Kupnicka D, Kubicka-Wołkowska J, Pluta A, Brzozowski K, Potemski P, et al. SMAC protein expression as a potent favorable prognostic factor in locally advanced breast cancer. Pol J Pathol. 2018;69(1):33–41.
- Waks AG, Desai Nv, Li T, Poorvu PD, Partridge AH, Sinclair N, et al. A prospective trial of treatment de-escalation following neoadjuvant paclitaxel/trastuzumab/pertuzumab in HER2-positive breast cancer. NPJ Breast Cancer. 2022;8(1):63.
- Wu Y, Zhong R, Ma F. HER2-low breast cancer: Novel detections and treatment advances. Crit Rev Oncol Hematol. 2023:181:103883.
- Zhu J, Jiao D, Wang C, Lu Z, Chen X, Li L, et al. Neoadjuvant efficacy of three targeted therapy strategies for HER2-positive breast cancer based on the same chemotherapy regimen. Cancers (Basel). 2022;14(18):4508.
- Wang Q, Wang X, Yang Y. Advances in neoadjuvant therapy for HER2-positive breast cancers: a narrative review. Gland Surg. 2022;11(8):1415–1423.
- Nodehi RS, Kalantari B, Raafat J, Ansarinejad N, Moazed V, Mortazavizadeh SMR, et al. A randomized, double-blind, phase III, non-inferiority clinical trial comparing the efficacy and safety of TA4415V (a proposed trastuzumab biosimilar) and Herceptin (trastuzumab reference product) in HER2-positive early-stage breast cancer patients. BMC Pharmacol Toxicol. 2022;23(1):57.
- Zhang J, Yu Y, Lin Y, Kang S, Lv X, Liu Y, et al. Efficacy and safety of neoadjuvant therapy for HER2-positive early breast cancer: a network meta-analysis. Ther Adv Med Oncol. 2021:13:17588359211006948.
- Lau KH, Tan AM, Shi Y. New and emerging targeted therapies for advanced breast cancer. Int J Mol Sci. 2022;23(4):2288.
- Hirmas N, Holtschmidt J, Loibl S. Shifting the paradigm: the transformative role of neoadjuvant therapy in early breast cancer. Cancers (Basel). 2024;16(18):3236.
- Potter S, Avery K, Ahmed R, de Boniface J, Chatterjee S, Dodwell D, et al. Protocol for the development of a core outcome set and reporting guidelines for locoregional treatment in neoadjuvant systemic breast cancer treatment trials: the PRECEDENT project. BMJ Open. 2024;14(4):e084488.
- Hyder T, Bhattacharya S, Gade K, Nasrazadani A, Brufsky AM. Approaching neoadjuvant therapy in the management of early-stage breast cancer. Breast Cancer (Dove Med Press). 2021:13:199–211.
- Blohmer JU, Link T, Reinisch M, Just M, Untch M, Stötzer O, et al. Effect of denosumab added to 2 different nab-paclitaxel regimens as neoadjuvant therapy in patients with primary breast cancer: the GeparX 2 × 2 randomized clinical trial.JAMA Oncol. 2022;8(7):1010–1018.
- Jiang M, Chai Y, Liu J, He M, Wang Y, Yang X, et al. Neoadjuvant inetetamab and pertuzumab with taxanes and carboplatin (TCbIP) In locally advanced HER2-positive breast cancer: a prospective cohort study with propensity-matched analysis. BMC Cancer. 2024;24(1):877.
- Golshan M, Loibl S, Wong SM, Houber JB, O’Shaughnessy J, Rugo HS, et al. Breast conservation after neoadjuvant chemotherapy for triple-negative breast cancer: surgical results from the BrighTNess randomized clinical trial.JAMA Surg. 2020;155(3):e195410.
- Untch M, Fasching PA, Konecny GE, Hasmuller S, Lebeau A, Kreienberg R, et al. Pathologic complete response after neoadjuvant chemotherapy plus trastuzumab predicts favorable survival in human epidermal growth factor receptor 2-overexpressing breast cancer: Results from the TECHNO trial of the AGO and GBG study groups. J Clin Oncol. 2011;29(25):3351–3357.
- De Luca A, Frusone F, Buzzacchino F, Amabile MI, Taffurelli M, del Mastro L, et al. First Surgical National Consensus Conference of the Italian Breast Surgeons association (ANISC) on breast cancer management in neoadjuvant setting: Results and summary. Eur J Surg Oncol. 2021;47(8):1913–1919.
- Weber WP, Matrai Z, Hayoz S, Tausch C, Henke G, Zimmermann F, et al. Association of axillary dissection with systemic therapy in patients with clinically node-positive breast cancer. JAMA Surg. 2023;158(10):1013-1021.
- Magbanua MJM, Brown Swigart L, Ahmed Z, Sayaman RW, Renner D, Kalashnikova E, et al. Clinical significance and biology of circulating tumor DNA in high-risk early-stage HER2-negative breast cancer receiving neoadjuvant chemotherapy. Cancer Cell. 2023;41(6):1091-1102.e4.
- Crocamo S, Binato R, de Paula B, Vignal G, Magalhães L, Sarmento R, et al. Neoadjuvant zoledronic acid for HER2-positive breast cancer: the Zo-NAnTax trial. Ther Adv Med Oncol. 2019:11:1758835919853971.
- Chou HH, Kuo WL, Yu CC, Tsai HP, Shen SC, Chu CH, et al. Impact of age on pathological complete response and locoregional recurrence in locally advanced breast cancer after neoadjuvant chemotherapy. Biomed J. 2019;42(1):66-74.
- Wang BC, Fu C, Xie LK, Kuang BH, Zhao YX. Comparative toxicities of neoadjuvant chemotherapy with or without bevacizumab in HER2-negative breast cancer patients: a meta-analysis. Ann Pharmacother. 2020;54(6):517–525.
- Yin G, Zhao L. Risk of hypertension with anti-VEGF monoclonal antibodies in cancer patients: a systematic review and meta-analysis of 105 phase II/III randomized controlled trials. J Chemother. 2022;34(4):221–234.
- Brown JC, Huedo-Medina TB, Pescatello LS, Pescatello SM, Ferrer RA, Johnson BT. Efficacy of exercise interventions in modulating cancer-related fatigue among adult cancer survivors: A meta-analysis. Cancer Epidemiol Biomarkers Prev. 2011;20(1):123–133
- Zamorano JL, Lancellotti P, Rodriguez Muñoz D, Aboyans V, Asteggiano R, Galderisi M, et al. 2016 ESC position paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: the Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(36):2768–2801.
- Zhu X, Shen J, Zhang H, Wang X, Zhang H, Yu J, et al. A novel combined nomogram model for predicting the pathological complete response to neoadjuvant chemotherapy in invasive breast carcinoma of no specific type: Real-world study. Front Oncol. 2022:12:916526.
- Park JW, Liu MC, Yee D, Yau C, van ’t Veer LJ, Symmans WF, et al. Adaptive randomization of neratinib in early breast cancer. N Engl J Med. 2016;375(1):11–22.
- Hatschek T, Foukakis T, Bjöhle J, Lekberg T, Fredholm H, Elinder E, et al. Neoadjuvant trastuzumab, pertuzumab, and docetaxel vs trastuzumab emtansine in patients with ERBB2-positive breast cancer: A phase 2 randomized clinical trial.JAMA Oncol. 2021;7(9):1360–1367.
- Tian C, Wang M, Liu H, Liu J, Xu M, Ma L. Efficacy and safety of neoadjuvant pyrotinib plus docetaxel/liposomal doxorubicin/cyclophosphamide for HER2-positive breast cancer. Ir J Med Sci. 2023;192(3):1041–1049.
- Pérez-García JM, Cortés J, Ruiz-Borrego M, Colleoni M, Stradella A, Bermejo B, et al. 3-year invasive disease-free survival with chemotherapy de-escalation using an 18F-FDG-PET-based, pathological complete response-adapted strategy in HER2-positive early breast cancer (PHERGain): a randomised, open-label, phase 2 trial. Lancet. 2024; 403(10437):1649–1659.
- Liu Z, Wang C, Chen X, Zhu J, Sun X, Xia Q, et al. Pathological response and predictive role of tumour-infiltrating lymphocytes in HER2-positive early breast cancer treated with neoadjuvant pyrotinib plus trastuzumab and chemotherapy (Panphila): a multicentre phase 2 trial. Eur J Cancer. 2022:165:157–168.
- Baselga J, di Cosimo S, Fauria K, Baselga J, Bradbury I, Eidtmann H, et al. Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): a randomised, open-label, multicentre, phase 3 trial. Lancet. 2012;379(9816):633–640.
- Nitz UA, Gluz O, Christgen M, Grischke EM, Augustin D, Kuemmel S, et al. De-escalation strategies in HER2-positive early breast cancer (EBC): Final analysis of the WSG-ADAPT HER2+/HR- phase II trial: Efficacy, safety, and predictive markers for 12 weeks of neoadjuvant dual blockade with trastuzumab and pertuzumab ± weekly paclitaxel. Ann Oncol. 2017;28(11):2768–2772.
- Loibl S, André F, Bachelot T, et al. Early breast cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2024;35(2):159–182.
- Mercogliano MF, Bruni S, Mauro FL, Schillaci R. Emerging Targeted Therapies for HER2-Positive Breast Cancer. Cancers (Basel). 2023;15(7):1987.
- Lin NU, Murthy RK, Abramson V, Anders C, Bachelot T, Bedard PL, et al. Tucatinib vs placebo, both in combination with trastuzumab and capecitabine, for previously treated ERBB2 (HER2)-positive metastatic breast cancer in patients with brain metastases: Updated exploratory analysis of the HER2CLIMB randomized clinical trial. JAMA Oncol. 2023;9(2):197–205.
- Loi S, Giobbie-Hurder A, Gombos A, Bachelot T, Hui R, Curigliano G, et al. International Breast Cancer Study Group and the Breast International Group. Pembrolizumab plus trastuzumab in trastuzumab-resistant, advanced, HER2-positive breast cancer (PANACEA): a single-arm, multicentre, phase 1b-2 trial. Lancet Oncol. 2019;20(3):371–382.
- Hashem M, Rehman S, Salhab M. The Role of Human Epidermal Growth Factor Receptor 2 (HER2)-Targeted Therapies in Early-Stage Breast Cancer: Current Practices, Treatment De-escalation, and Future Prospects. Cureus. 2024;16(2):e55230.
- Wuerstlein R, Harbeck N. Neoadjuvant Therapy for HER2-positive Breast Cancer. Rev Recent Clin Trials. 2017;12(2):81–92.
- Duro-Snchez S, Alonso M, Arribas J. Immunotherapies against HER2-Positive Breast Cancer. Cancers (Basel). 2023;15(4):1069.
- Barot SV, Roesch E, Abraham J. Optimizing adjuvant and post-neoadjuvant therapy in HER2-positive early breast cancer. Expert Rev Anticancer Ther. 2022;22(12):1289–1299.
- Gianni L, Bianchini G. Abstract ED11-2: HER2 positive breast cancer. Cancer Res. 2023;83(5_Supplement): ED11–12.
- Angelis V, Okines AFC. Systemic Therapies for HER2-Positive Advanced Breast Cancer. Cancers (Basel). 2023;16(1):23.
- Dowling G, Keelan S, Toomey S, Daly G, Hennessy B, Hill A. Review of the status of neoadjuvant therapy in HER2-positive breast cancer. Front Oncol. 2023;13:1066007.
Cite this article
Auricchio P, Mayr C, Polato R, Frena A. The Role of Neoadjuvant Treatment in HER-2 Positive Breast Cancer: What a Surgeon Should Know. Clin Surg J. 2026;7(1):1–8.
Keywords
HER2-positive; Neoadjuvant therapy; Breast-conserving surgery; Trastuzumab; Pertuzumab; pCR; Axillary surgery; Targeted therapy
Copyright
© 2026 Pasquale Auricchio. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
