Impact of Initial Resectability and Neoadjuvant Chemotherapy on Overall Survival for Pancreatic Adenocarcinoma
* Katherine E Poruk;
David Hyman;
Alfredo Verastegui Davila;
Mary Tice and John A Stauffer;
-
* Katherine E Poruk: Department of General Surgery, The Mayo Clinic, Jacksonville, FL 32224, USA
-
David Hyman: Department of General Surgery, The Mayo Clinic, Jacksonville, FL 32224, USA
-
Alfredo Verastegui Davila: Department of General Surgery, The Mayo Clinic, Jacksonville, FL 32224, USA
-
Mary Tice and John A Stauffer: Department of General Surgery, The Mayo Clinic, Jacksonville, FL 32224, USA
Abstract
Introduction: Surgical resection offers the best chance of long-term survival for patients with Pancreatic adenocarcinoma (PDAC). Neoadjuvant Chemotherapy (NAC) is increasingly utilized for the treatment of occult distant metastases and to improve tumor resectability, but questions remain about optimal patient selection for NAC. We sought to evaluate the impact of initial tumor resectability and neoadjuvant chemotherapy on overall survival after resection.
Methodology: A retrospective review was performed for patients who underwent PDAC resection between January 2010 and December 2020 at a tertiary hospital. Overall Survival (OS) was assessed using the Kaplan-Meier method and univariate and multivariate Cox models, both based on the date of initial tumor diagnosis.
Results: Between 2010 and 2020, 356 patients underwent PDAC resection. NAC was administered to 129 patients (36%), while the remaining 227 patients (64%) underwent resection without NAC. 254 patients (71%) were classified as initially resectable, with a higher percentage going for upfront surgery versus NAC (92% patients vs. 35% patients, P < 0.001). Median OS was not significantly different between patients who underwent NAC vs. upfront surgery (P = 0.59) or between those with initial resectability vs. BL/LA (P = 0.25) in this cohort. By multivariate analysis, positive lymph nodes (P = 0.006) and T3/T4 tumors (P = 0.008) were independent predictors of poor survival, while adjuvant chemotherapy was associated with improved survival (P < 0.001). When stratified by initial resectability and neoadjuvant chemotherapy, the highest median OS was seen in resectable patients who received neoadjuvant treatment (68.8 months), while the worst was in resectable patients who did not receive neoadjuvant chemotherapy (22 months). Initially, borderline resectable or locally advanced patients who underwent neoadjuvant chemotherapy had similar survival to resectable patients that did not (32.7 vs. 31 months).
Conclusion: In a selected retrospective cohort, neither NAC nor initial resectability was associated with improved median OS, suggesting that histopathologic and biologic factors play a role. NAC may still improve survival in resectable patients and plays an important role in converting patients with nonresectable disease to resectable disease.
Introduction
Pancreatic Ductal Adenocarcinoma (PDAC) is a leading cancer diagnosis in the United States, and is estimated to be a top cause of cancer death in the next several decades [1]. While survival has slowly improved over the last several years, overall five-year survival remains dismal at 13% across all stages of disease [1]. In many situations, this is related to the late stage at which most patients are diagnosed, as only 20%–30% present with PDAC at a stage when they may be surgical candidates. Surgical resection offers the best chance for meaningful long-term survival but is restricted to patients without distant metastases who have resectable tumors [2,3]. Even with surgery, the majority of patients will recur with distant disease within 3 years [4]. As a result, optimal treatment of PDAC involves combining surgery with chemotherapy and potentially radiation therapy for the best chance of cure, with specific decisions about treatment often stratified based on clinical factors to predict the risk of tumor recurrence.
Nearly all patients receive chemotherapy at some point in PDAC treatment, given the aggressiveness of the disease. Chemotherapy offers the ability to kill microscopic tumor cells that have the potential to spread to other organs through lymphatic and perineural tissue. However, controversy remains as to the best time to offer chemotherapy in conjunction with surgical resection. Neoadjuvant Chemotherapy (NAC) is given to patients prior to surgical resection. National guidelines recommend NAC to patients with tumors involving the nearby portal vein and/or hepatic arteries, often termed “Borderline Resectable” (BR) or “Locally Advanced” (LA), in order to shrink the tumor and increase the likelihood of surgical resection [5]. However, some institutions routinely recommend NAC to all patients with PDAC, even if the tumor appears resectable upfront. Proponents of this argue that NAC increases the likelihood of microscopic complete tumor resection and can identify patients with poor tumor biology that may recur quickly after an operation, thus sparing these patients the morbidity and mortality associated with surgery [6–8]. Furthermore, patients may tolerate upfront chemotherapy better, and surgical complications can delay the timely receipt of postoperative chemotherapy [9]. Other centers, and even patients, favor upfront surgery for resectable tumors, followed by adjuvant chemotherapy 4 weeks–6 weeks later. Several studies have demonstrated improved disease-free and overall survival in patients receiving chemotherapy after resection compared with observation alone [10,11]. At this time, controversy remains as to who should receive NAC, and the decision to administer is often based not only upon tumor characteristics but also upon patient comorbidities and even patient and surgeon preference. Prospective randomized clinical trials are underway to potentially determine if NAC should be administered in all patients with PDAC [12].
Until this data has resulted, the decision regarding surgery or NAC is often at the discretion of the patient, the surgeon, and the treating oncologist. The aim of this study was to evaluate the impact of initial tumor resectability and NAC on overall survival.
Methodology
Patient Selection and Data Collection: Data were retrospectively collected from January 2010 to December 2020 for all patients undergoing PDAC resection at the Mayo Clinic in Florida. Charts were reviewed, and information on patient demographics, surgical treatment, chemoradiation therapy, perioperative characteristics, and tumor characteristics was collected. All resected cancers were reviewed by a pathologist at the time of surgery, and included an analysis of TNM tumor stage, grade, margin status, nodal status, and the presence of perineural and/or perivascular invasion. Overall survival was calculated from the date of cancer diagnosis by imaging or tumor biopsy to the date of last follow-up or death. This allowed for the removal of any potential lead time bias in patients who received chemotherapy prior to surgery. The administration of neoadjuvant and/or adjuvant chemotherapy and the specific treatment regimen were at the discretion of the treating medical and surgical oncologist and were not affected by this study. At least 3 months of chemotherapy was administered in all patients who underwent neoadjuvant therapy, with FOLFIRINOX being the preferred treatment when possible. The study was carried out with the approval of the Mayo Clinic Institutional Review Board (IRB).
Statistical Analysis: Statistical analysis was performed using Stata 13 (StataCorp, College Station, TX). A P-value less than 0.05 was considered significant. Summary statistics for the entire population and each cohort were presented as mean variables with ranges for continuous variables and percentages and frequencies for categorical variables. Differences between continuous variables were assessed by Student’s t-test, and categorical variables were analyzed by Fisher’s exact test. Median overall survival and differences in survival were calculated by the Kaplan-Meier method and the Cox-Mantel log-rank test.
Results
Patient Demographics: During the study period, 356 patients underwent surgical resection for PDAC (Table 1). The average age at surgery was 69.2 years (range, 40 years to 91 years), and 187 patients (53%) were male. Of the 356 patients, 129 (36%) received NAC at the discretion of their medical and surgical oncologist treatment. This included 70 patients (54%) who received FOLFIRINOX, 40 patients (31%) who received gemcitabine-based chemotherapy, 1 patient (1%) who received capecitabine-based chemotherapy, and the remaining 18 patients (14%) who received a different or unknown chemotherapy agent. All patients underwent surgical resection. Median overall survival from the time of tumor diagnosis for the entire patient cohort was 29.7 months.
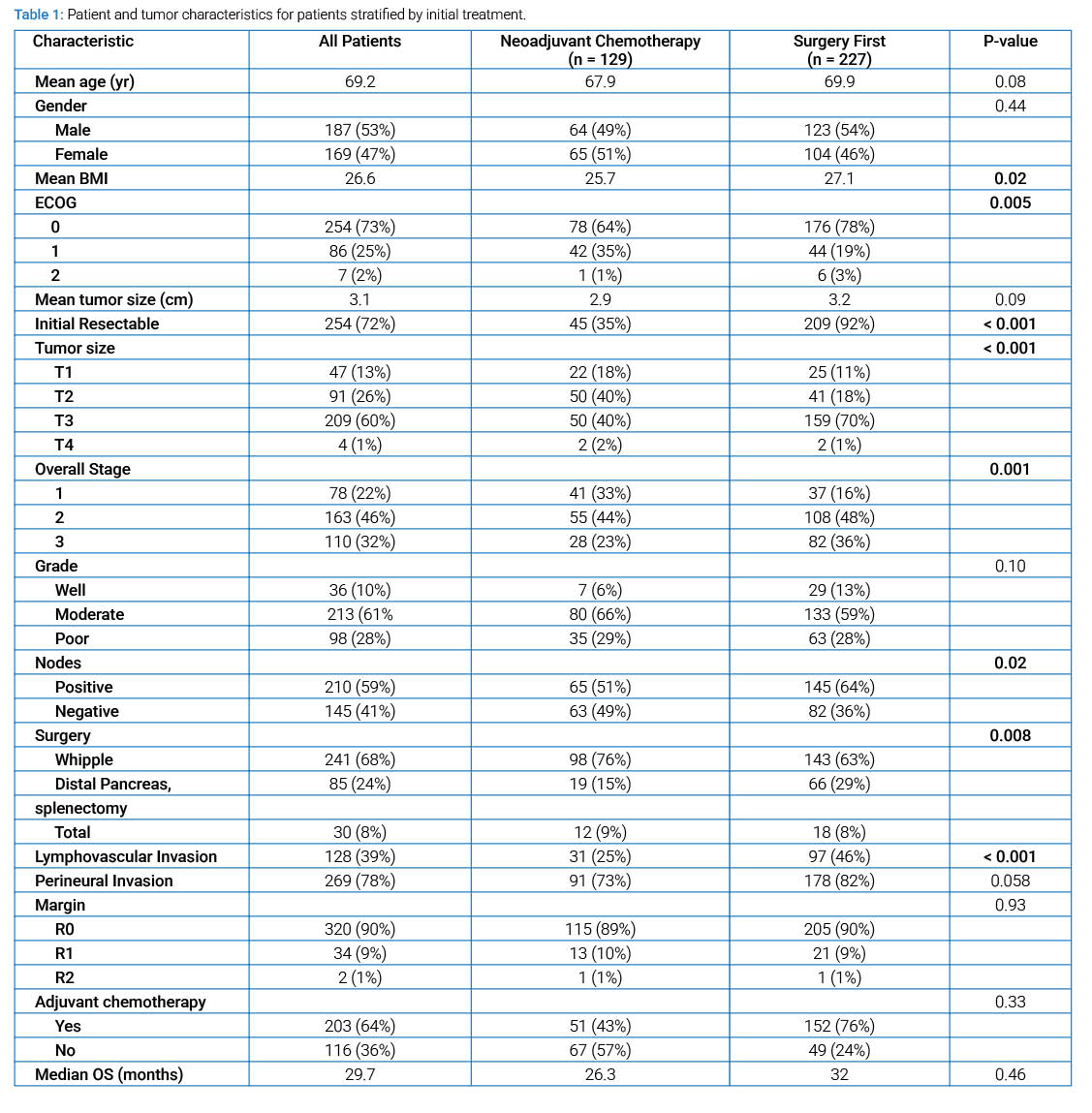
Patient demographics and perioperative characteristics are given for patients depending on treatment with or without NAC (Table 1). There was no difference in mean age at surgery or gender between the two groups. Patients who were treated with upfront resection tended toward a lower ECOG compared to those receiving NAC, while those with resectable tumors on radiology were more likely to proceed with surgery first (P < 0.05, both). Patients who required a Whipple operation were also more likely to undergo NAC first (76% vs. 63%) compared to those who required a distal pancreatectomy (15% vs. 29%) (P = 0.008). By histopathology, patients who did not receive NAC tended to have larger mean tumor size (3.2 cm vs. 2.9 cm, P = 0.09). and a higher rate of positive lymph nodes at the time of operation (64% vs. 51%, P = 0.02). However, there was no difference in tumor grade or margin status at surgery. Additionally, patients who underwent upfront resection were more likely to receive adjuvant chemotherapy than those who received NAC (75% vs. 43%, P < 0.01). Median overall survival, calculated from the time of diagnosis, was similar between patients who received NAC compared to those who did not (26.3 months vs. 32.0 months, P = 0.46) (Figure 1).
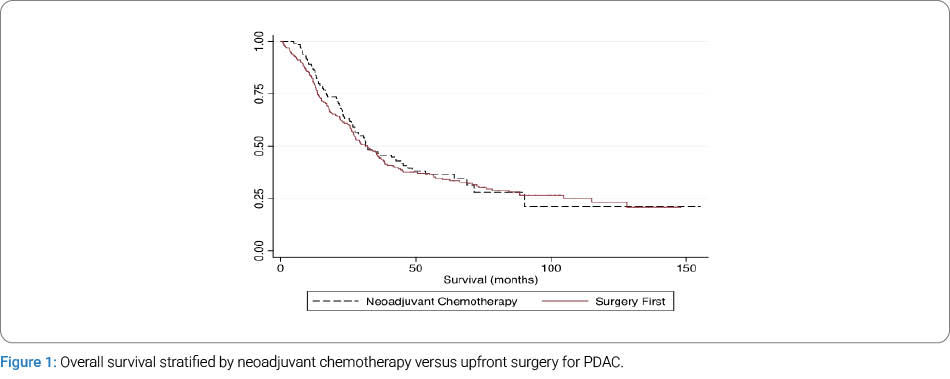
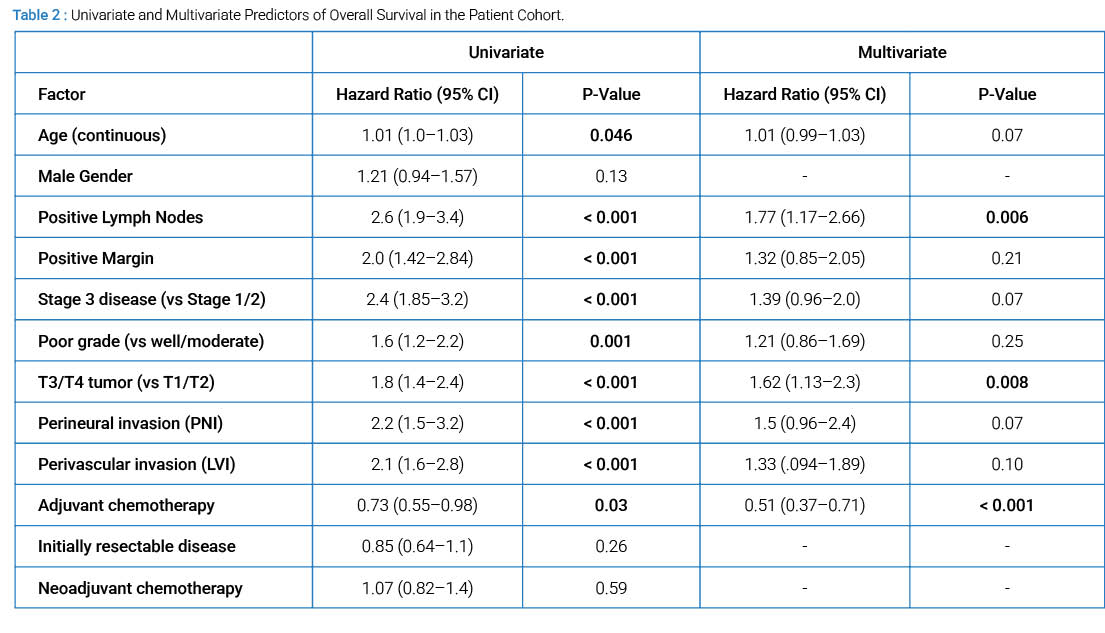
Predictors of Overall Survival: A univariate analysis was performed to determine predictors of overall survival (Table 2). Older age as a continuous variable, positive lymph nodes, a positive surgical margin, poor tumor grade, stage 3 disease, T3 or T4 tumors, perineural invasion, and perivascular invasion were all associated with worse OS (P < 0.05, all). The receipt of adjuvant chemotherapy was associated with improved OS (P < 0.05). NAC was not associated with improved OS (Figure 1). On multivariate analysis, only positive lymph nodes and T3 or T4 tumors remained significant predictors of worse OS, while the receipt of adjuvant chemotherapy was associated with improved OS (P < 0.05, all).
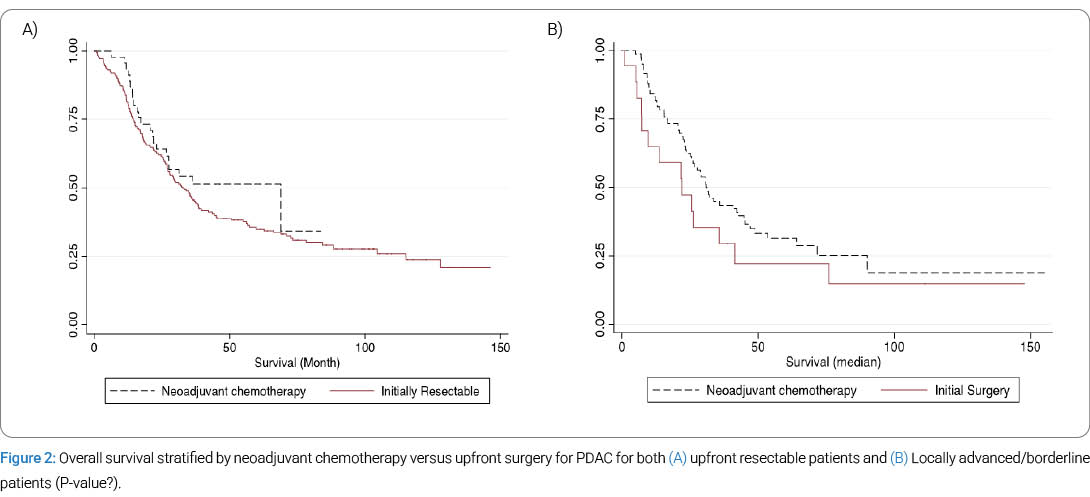
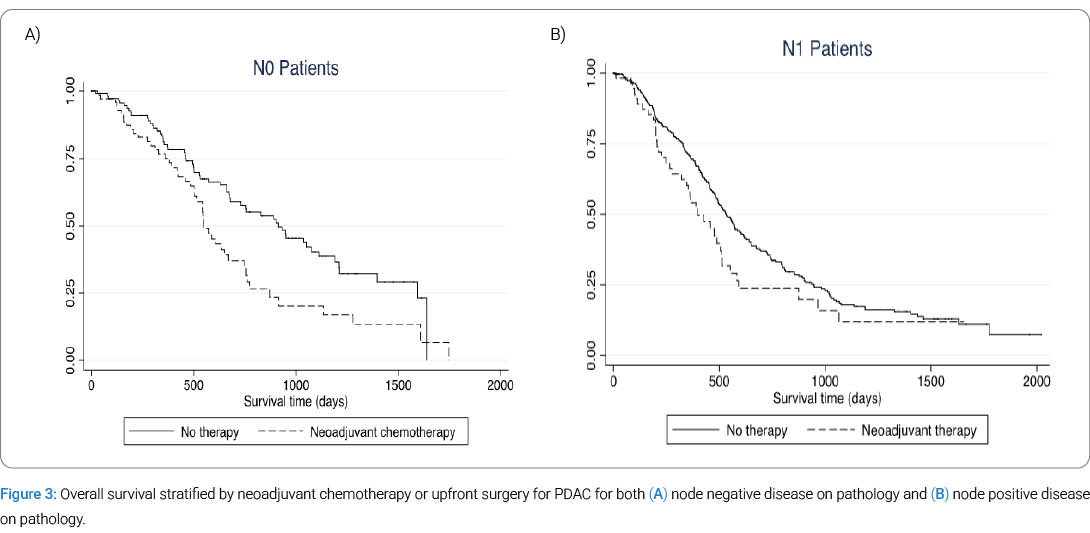
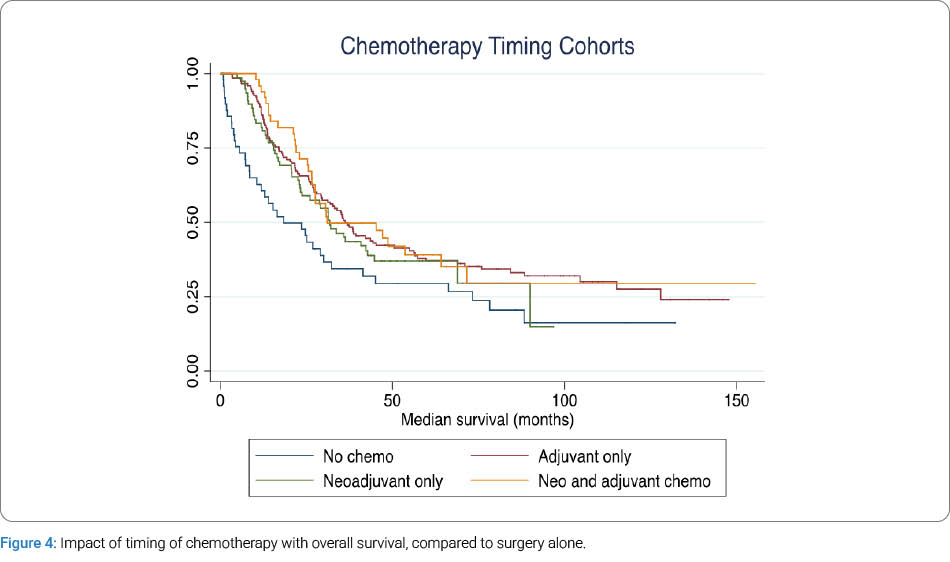
We also evaluated OS when stratified by upfront resectable patients or borderline/locally advanced patients (Figure 2). OS survival was not significantly different for upfront resectable patients based on treatment (P = 0.22) or borderline resectable/locally advanced patients based on treatment (P = 0.17). We further analyzed overall survival stratified by treatment and node status at the time of surgery. Improved OS was seen for patients with node-negative disease who did not receive NAC (median survival, 30 months vs. 18 months, P = 0.006) (Figure 3). Improved OS was also seen for patients with node-positive disease who underwent surgery first (median survival, 17.5 months vs. 13.0 months, P = 0.05) (Figure 3). Improved survival was observed in all patients who received chemotherapy, either before or after surgery, compared with those who underwent surgery alone (Figure 4).
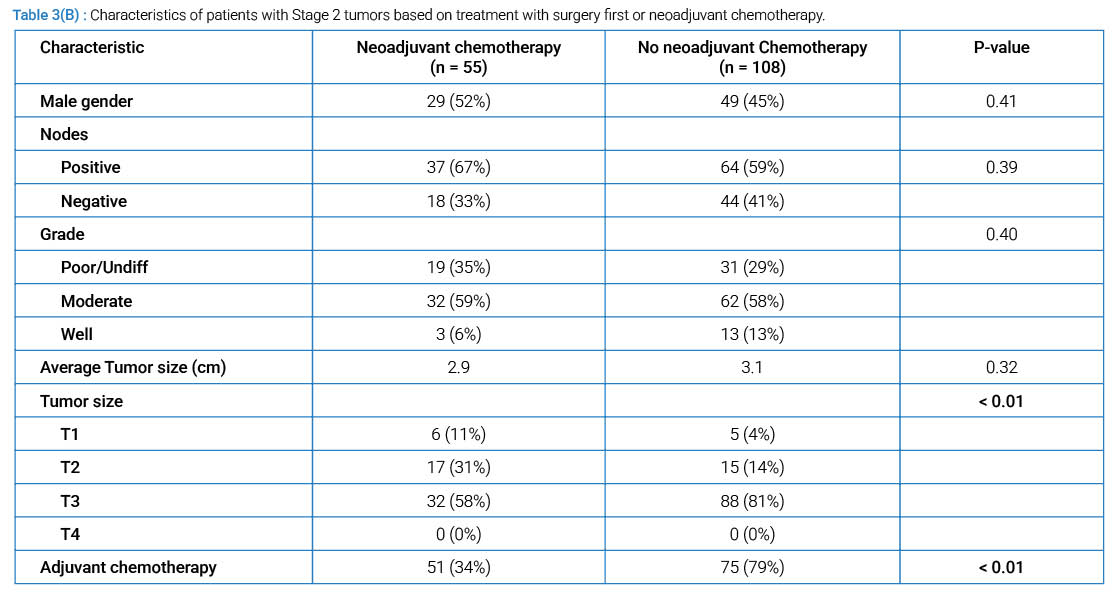
Survival by Overall Stage: Patient demographics and perioperative characteristics are given for patients depending on treatment with or without neoadjuvant chemotherapy and split by overall TNM stage for both stage I and stage II patients (Table 3A, Table 3B), in order to evaluate the impact of NAC on early-stage tumors. Of note, five patients had a complete response after chemotherapy and were given a stage 0 diagnosis, while stage III disease was diagnosed in 110 patients who underwent operative resection, including 82 patients who received NAC.
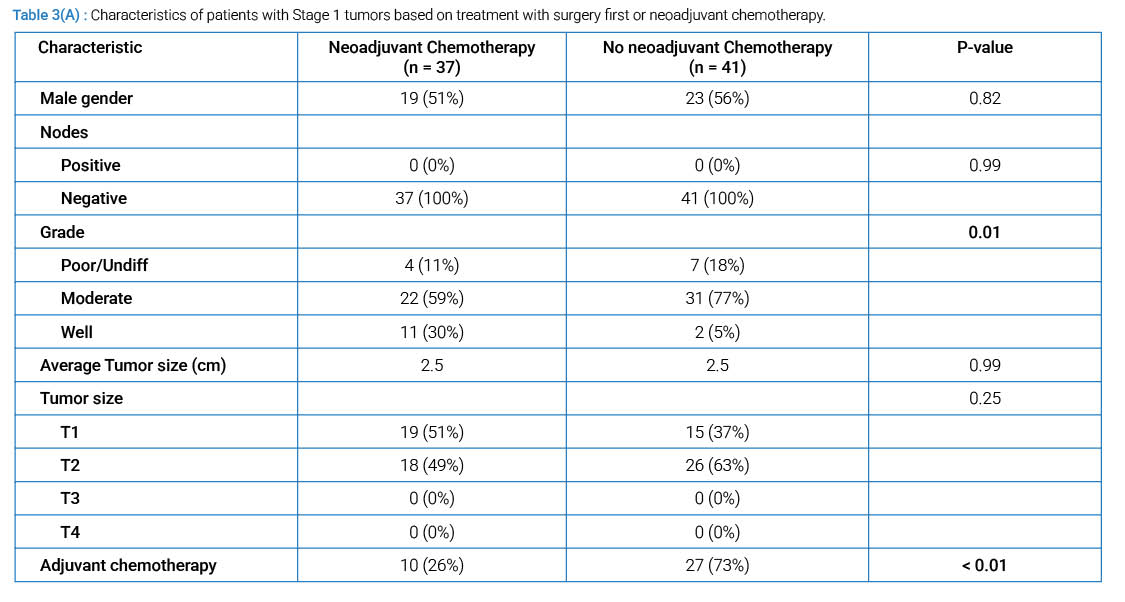
Seventy-eight patients (23%) had stage I disease based on TNM stage, and 41 patients received NAC. There was no significant difference in age or gender between Stage I patients who received adjuvant chemotherapy. For patients with Stage I disease based on histopathological assessment at the time of surgery, tumor grade differed between the groups, but there was otherwise no difference in grade, lymph node status, or tumor size. Patients who first underwent surgery were more likely to receive adjuvant chemotherapy (P < 0.01). Median overall survival for patients with stage I disease who underwent NAC was significantly shorter than that of patients who did not (18.0 months vs. 36.5 months, P = 0.004).
Stage II disease was diagnosed in 163 patients (46%), including 55 patients who received NAC (Table 2). There was no significant difference in age or gender between Stage II patients who received adjuvant chemotherapy. Patients who underwent NAC were significantly more likely to have a lower T-stage, but there was no difference in average tumor size, tumor grade, or positive lymph nodes on pathology. Patients who first underwent surgery were more likely to receive adjuvant chemotherapy (P < 0.01). Median overall survival for patients with stage II disease was significantly shorter in patients who underwent NAC (16.5 months vs. 18.4 months, P = 0.04).
Discussion
Pancreatic cancer remains a difficult disease to effectively treat, given the high risk of systemic recurrence. Surgery offers the best chance for meaningful long-term survival and even cure, but the majority of surgical patients will recur with distant disease within 3 years of an operation [2,3]. This creates a strong need for a multimodal approach to PDAC treatment, including.
improved methods to stratify patients at highest risk for recurrence to chemotherapy and radiation therapy. In addition, the decision to offer additional adjuvant chemotherapy is often based upon the histopathology of a tumor at the time of surgical resection. However, this can be difficult to assess accurately in patients who have responded to NAC, which can shrink the tumor and eradicate nodal disease.
Several significant differences were noted in the demographics of patients who underwent NAC compared with those who underwent immediate surgery. Patients who received NAC had a higher ECOG than patients who underwent surgery first. This may have been to give time to assess a tumor’s biology prior to undergoing a major pancreas operation, given the potential risk of morbidity and mortality. In addition, patients who underwent NAC were more likely to have smaller tumors at the time of surgical resection, likely related to a treatment effect in which the chemotherapeutic agent was able to successfully shrink the tumor. Similarly, patients undergoing NAC were less likely to have positive lymph nodes detected at the time of surgery, which was also likely due to the treatment effect. None of these differences were unexpected and reflected the benefits that NAC can often provide prior to surgery, namely decreasing tumor burden to allow for resection, but can also cause the confounding issue of stage migration when comparing by stage.
This study highlights the survival differences based on overall TNM stage, tumor size, and nodal status stratified by the receipt of NAC. Patients who underwent NAC had significantly decreased median survival after surgery compared to patients who did not receive preoperative therapy, both overall and in several of the categories identified, including node-negative (N0) disease, node-positive (N1) disease, or early-stage disease (1 or 2). Interestingly, this was despite the fact that in all demographic groups, patients who underwent NAC were more likely to have factors independently associated with better survival, such as smaller tumor size or negative lymph nodes. This does not suggest that NAC is associated with poor survival; rather, TNM staging may not accurately predict overall survival based solely on stage, particularly when neoadjuvant therapies are considered. Survival is likely based on stage at diagnosis for patients who undergo NAC rather than the stage based on histopathology at surgery, and should be recognized when considering a patient for additional postoperative chemotherapy. In addition, this study demonstrated the importance of receiving chemotherapy at any point (either before or after surgery), as patients who did not receive any chemotherapy had the worst survival.
There are several limitations to this study. First, this study is a retrospective review, which has the potential to underestimate certain variables, including the rate of adjuvant chemotherapy in patients who choose to receive follow-up care at an institution closer to their home. Furthermore, the specific NAC administered was decided upon by an individual’s medical oncologist, and the wide variety of chemotherapeutic agents used may create an unidentified bias in overall survival. Additionally, no survival data were available for patients with unresectable or locally advanced tumors that underwent NAC but did not respond sufficiently to allow for surgical resection. It is likely that compared to this group, patients who underwent NAC and subsequent resection would demonstrate a significant survival benefit.
In conclusion, this study assessed the ability of the TNM staging system based on histopathology at the time of surgical resection to predict overall survival in patients with PDAC receiving NAC. Patients who underwent NAC had significantly decreased overall median survival compared to patients going straight to surgery, including when stratified by tumor size, nodal status, and overall stage. Survival is likely based upon stage at diagnosis and not at resection for patients undergoing NAC. Surgeons should be aware that patients with negative nodes or small tumor size after NAC and surgical resection should still be encouraged to receive adjuvant chemotherapy. Future studies are needed to determine the most predictive methods for assessing and predicting overall survival in patients receiving neoadjuvant chemotherapy.
Author Contributions
Katherine E Poruk and John A Stauffer conceived of the study design and hypothesis. Katherine E Poruk performed statistical analysis and interpretation, including calculation of survival as defined in the study protocol. Katherine E Poruk, David Hyman, Alfredo Verastegui Davila, and Mary Tice performed data collection and manuscript preparation. All authors provided critical analysis and approval of the manuscript.
Conflict of Interest
The authors of this study have no disclosures to report. The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
References
- Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin 2025;75(1):10–45.
- Sener SF, Fremgen A, Menck HR, Winchester DP. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985-1995, using the National Cancer Database. J Am Coll Surg. 1999;189(1):1–7.
- Bilimoria KY, Bentrem DJ, Ko CY, Stewart AK, Winchester DP, Talamonti MS. National failure to operate on early stage pancreatic cancer. Ann Surg. 2007;246(2):173–180.
- Dunne RF, Hezel AF. Genetics and biology of pancreatic ductal adenocarcinoma.HematolOncolClin N Am. 2015;29(4):595–608.
- Tempero MA, Arnoletti JP, Behrman SW, Ben-Josef E, 3rd Benson Al B, Casper ES, et al. Pancreatic Adenocarcinoma, version 2.2012: featured updates to the NCCN Guidelines. J NatlComprCancNetw. 2012;10(6):703–713.
- Palmer DH, Stocken DD, Hewitt H, Markham CE, Hassan AB, Johnson PJ, et al. A randomized phase 2 trial of neoadjuvant chemotherapy in resectable pancreatic cancer: gemcitabine alone versus gemcitabine combined with cisplatin. Ann Surg Oncol. 2007;14(7):2088–2096.
- Evans DB, Rich TA, Byrd DR, Cleary KR, Connelly JH, Levin B, et al. Preoperative chemoradiation and pancreaticoduodenectomy for adenocarcinoma of the pancreas. Arch Surg. 1992;127(11):1335–1339.
- Heinrich S, Pestalozzi BC, Schafer M, Weber A, Bauerfeind P, Knuth A, et al. Prospective phase II trial of neoadjuvant chemotherapy with gemcitabine and cisplatin for resectable adenocarcinoma of the pancreatic head. J ClinOncol. 2008;26(15):2526–2531.
- Wu W, He J, Cameron JL, Makary M, Soares K, Ahuja N, et al.The impact of postoperative complications on the administration of adjuvant therapy following pancreaticoduodenectomy for adenocarcinoma.Ann SurgOncol. 2014;21(9):2873–2881.
- Oettle H, Neuhaus P, Hochhaus A, Hartmann JT, Gellert K, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: the CONKO-001 randomized trial. JAMA. 2013;310(14):1473–1481.
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. 2004;350(12):1200–1210.
- Chawla A, Ferrone CR. Neoadjuvant therapy for resectable pancreatic cancer: an evolving paradigm shift. Front Oncol. 2019;17(9):1085.
Cite this article
Poruk KE, Hyman D, Davila AV, Tice M, Stauffer JA. Impact of initial resectability and neoadjuvant chemotherapy on overall survival for pancreatic adenocarcinoma. Clin Surg J. 2026;7(1):1–8.
Keywords
TNM stage; Neoadjuvant chemotherapy; Survival; Prognosis; Pancreatic adenocarcinoma; PDAC
Copyright:
© 2026 Katherine E Poruk. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
