Intestinal Obstruction: A Crisis to be Dealt With
Samia Mohan;
Priyanka Sharma;
Arjit Kapoor;
* Akshat Sudhanshu;
-
Samia Mohan: Department of General Surgery, Acharya Shri Chander College of Medical Sciences, Jammu and Kashmir, India.
-
Priyanka Sharma: Department of Microbiology, Government Medical College, Jammu and Kashmir, India.
-
Arjit Kapoor: Department of Surgery, Acharya Shri Chander College of Medical Sciences, Jammu and Kashmir, India.
-
* Akshat Sudhanshu: Department of Pediatric Surgery, All India Institute of Medical Sciences, Jammu, Jammu and Kashmir, India.
Abstract
Intestinal obstruction can involve small intestines or a large gut.
It is an emergency that needs immediate management to avoid serious complications like perforation leading to peritonitis, sepsis, and even death.
The most common cause of intestinal obstruction is post operative adhesions, but other common causes are hernias, worm bolus obstruction, volvulus, internal herniation and so on.
Introduction
Acute intestinal obstruction is usually caused by a mechanical cause but can also be caused by dynamic factors. Its incidence in patients who present to the emergency department is estimated at 2% to 8% [1–4].
The patient is usually dehydrated because of repeated vomitting, third-space loss, septic if presenyinglate, with distension, rapid pulse, low blood pressure, and absence of bowel sounds. Prompt and correct management plays a crucial role in deciding the patient’s future status. Adhesions cause 60 percent of cases [5].
Patients usually present with colicky pain, distension, and inability to pass feces or flats.
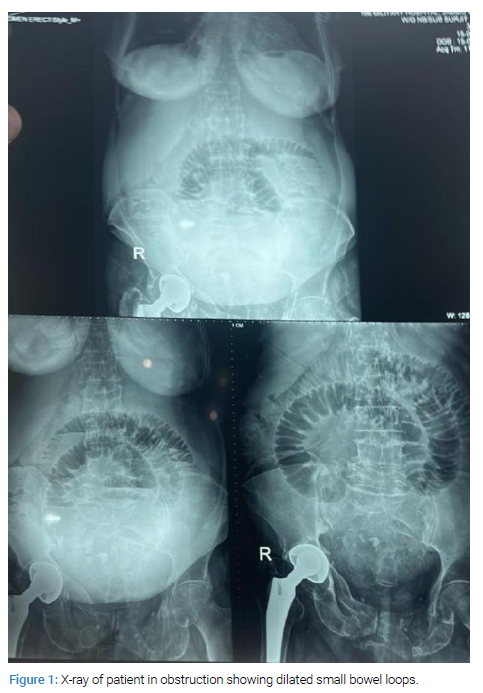
Abdominal plain X-ray is the first-level radiologic study (Figure 1). In small bowel obstruction, an X-ray of the abdomen is diagnostic in 50%–60% [6,7].
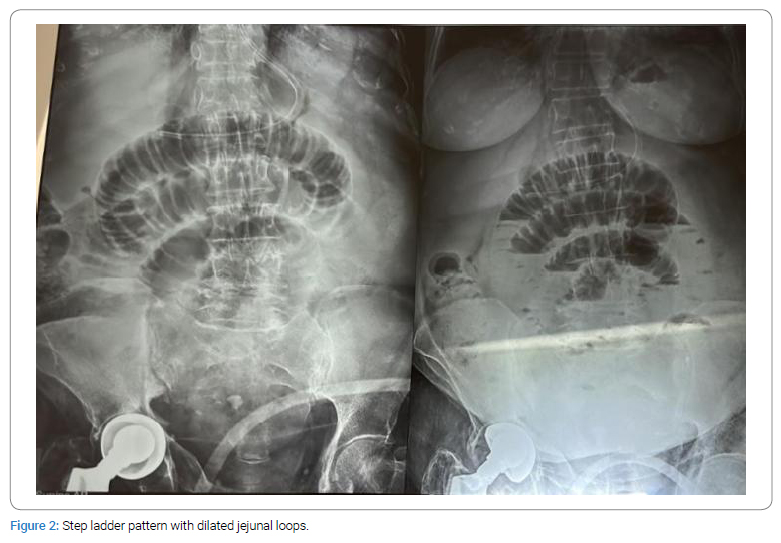
The typical picture of a step ladder pattern, prominent and distended bowel loops, and no air in the rectum are some features of obstruction (Figure 2).
In this study, we have studied all cases of intestinal obstruction that were presented to the surgery department of our hospital from January 2021 to December 2023.
Method
The study included all cases of intestinal obstruction admitted to our institution’s surgery department from January 2021 to December 2023.
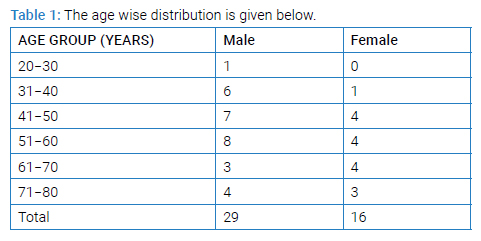
A total of 45 patients were admitted, out of which 29 were males and 16 were females (Table 1).
Results
Out of the total patients, 20 underwent exploratory laparotomy; 19 were managed conservatively. Out of 45 patients treated, six died. The total number of males was 29 and females were 16 (Table 2).
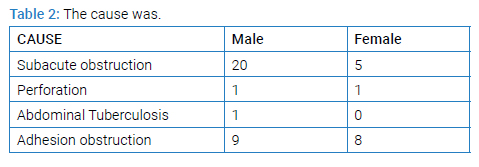
The most common cause of obstruction was adhesion obstruction.
Other causes were perforation, abdominal tuberculosis, and sub-acute obstruction, which were managed conservatively.
The patient was operated on after conservative management failed, and the cause was band obstruction. She had a history of cesarean sections in the past.
Discussion
This study showed the cases of intestinal obstruction that were presented to the surgery department of our institution and their management.
Intestinal obstruction is an emergency and needs proper management in order to reduce morbidity and mortality in these patients. It can dynamic or adynamic, depending on its cause.
The key is prompt diagnosis and treatment of the underlying cause.
Mortality ranges from 3% with simple obstruction to as much as 30% when there is vascular compromise/perforation of the obstructed intestine, despite improvements in diagnostic tools [8].
Initial management is intravenous fluids, antibiotics, correction of electrolytes, Ryle tube insertion, and Nil per orally (Figure 3).

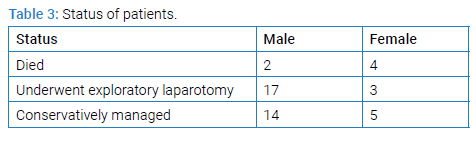
In case conservative management fails, then exploratory laparotomy is done, and the underlying cause is corrected to relieve the obstruction (Table 3).
Risk factors associated with high mortality were delay in diagnosis and presentation to Hospital, associated diseases such as diabetes, cardiac diseases, extremes of age, and patients with sepsis.
Conclusion
Intestinal obstruction, which can be small bowel or large bowel obstruction, is a common problem in emergencies requiring prompt diagnosis and management, either conservatively or, if need be, surgical.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
References
- ten Broek RPG, Issa Y, van Santbrink EJP, Bouvy ND, Kruitwagen RFPM, Jeekel J, et al. Burden of adhesions in abdominal and pelvic surgery: systematic review and meta-analysis. BMJ. 2013;347:f5588.
- Taylor MR, Lalani N. Adult small bowel obstruction. Acad Emerg Med. 2013;20(6):528–544.
- Miller G, Boman J, Shrier I, Gordon PH. Etiology of small bowel obstruction. Am J Surg. 2000;180(1):33–36.
- Barmparas G, Branco BC, Schnüriger B, Lam L, Inaba K, Demetriades D. The incidence and risk factors of post-laparotomy adhesive small bowel obstruction. J Gastrointest Surg. 2010;14(10):1619–1628.
- Shelton BK. Intestinal obstruction. AACN Clin Issues. 1999;10(4):478–491.
- Gans SL, Stoker J, Boermeester MA. Plain abdominal radiography in acute abdominal pain; past, present, and future. Int J Gen Med. 2012;5:525–533.
- Frager D. Intestinal obstruction role of CT. Gastroenterol Clin N Am. 2002;31(3):777–799.
- Sudarshan V, Husain JS, Choudhary KSS, Kumar NP. A study of surgical management of intestinal obstruction. International Surgery Journal. 2023;10(5):866–870.
Keywords
Intestinal obstruction; Dynamic obstruction
Cite this article
Mohan S, Sharma P, Kapoor A, Sudhanshu A. Intestinal obstruction: A crisis to be dealt with. Clin Surg J. 2024;5(1):1–3.
Copyright
© 2024 Akshat Sudhanshu. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
