Abstract
Acute cholecystitis in elderly and unfit patients is an increasingly common reason for hospital admission. It is often managed with percutaneous cholecystostomy. A 79-year-old lady who has Heart failure, AF, Diabetes and bed bound was admitted acute cholecystitis. She had abdominal Ultrasound (USG) confirming calculous cholecystitis and she was not fit for a cholecystectomy. There have various reports of creation of Cholecysto-duodenal fistula using covered metal stent to treat acute cholecystitis. They used multiple metallic stents to drain the biliary tree and created a cholecysto-enteric fistula using covered metal stent. A combined radiological and endoscopic approach has been used for placement of a cholecysto-duodenal stent using an 8 French ureteric stent successfully along with a percutaneous drain to drain the peri-cholecystitis abscess from gall bladder perforation.
Introduction
Acute cholecystitis in elderly and unfit patients is an increasingly common reason for hospital admission. It is often managed with percutaneous cholecystostomy. The drain in left in situ till there is a fibrous tractformed between the gall bladder and the skin and this may take up to 3 months. After removal of the drain this tract will slowly close with complete fibrosis of the tract. Some of these patients also have perforated gall bladder with peri-cholecystic collection making draining all the collections more challenging. In some patients these drains prevents rapid discharge back to residential care as care of the drain is not possible in many community settings. We describe a case where a combined percutaneous radiological and endoscopic trans-papillary approach was used successfully to stent the gall bladder via cystic duct in to the duodenum and at the same time peri-cholecystic abscess was drained with a percutaneous drain. Literature review has shown various methods been used for similarly cases however this is the first time this particular method has been reported.
Case Presentation
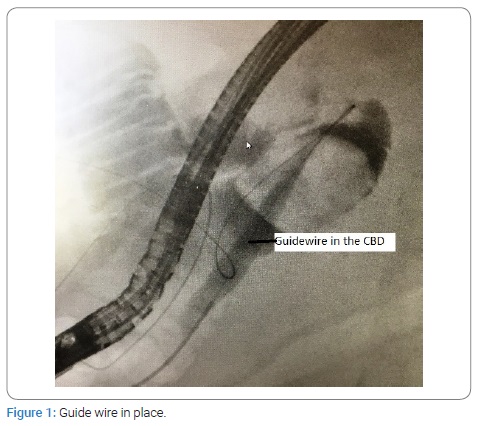
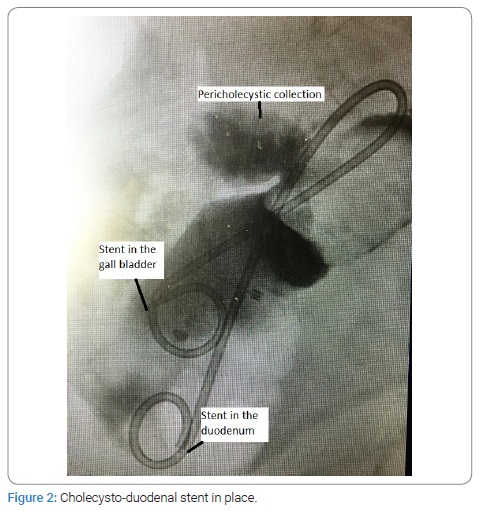
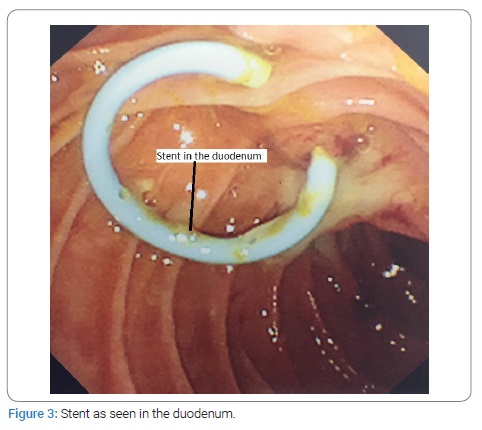
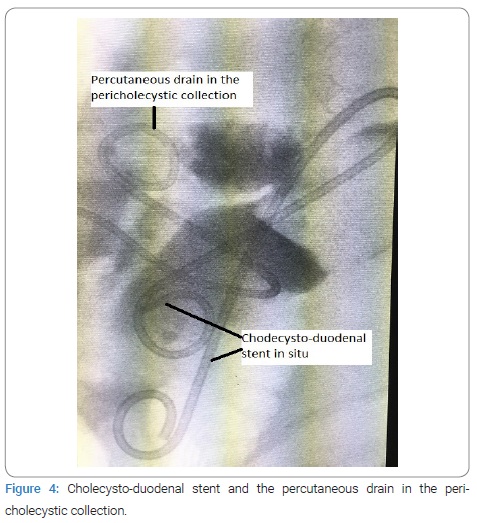
A 79-year-old lady who has Heart failure, AF, Diabetes and bed bound was admitted acute cholecystitis. She had abdominal Ultrasound (USG) confirming calculous cholecystitis and a subsequent Magnetic Resonance Cholangio-Pancreatography (MRCP) which showed a distended, thick walled gallbladder with stones and also a filling defect in the Common Bile Duct (CBD). She had a percutaneous cholecystostomy with initial clinical improvement. A tubogram subsequently confirmed forward flow of the contrast in to the bile duct and duodenum. We were unable to discharge her back to her residential care as they did not have the expertise to look after the percutaneous drains. She needed a permanent procedure to enable early removal of the percutaneous drain and discharge back to her residential care. She was not fit for a cholecystectomy. A decision was taken to attempt to drain the gall bladder in to the duodenum via cystic duct and common bile duct using a double J stent. Procedure was performed under propofol anaesthesia. A guide wire was passed under radiological guidance through the previous percutaneous drain in to the duodenumvia the cystic and common bile duct. This showed 2 large stones in the gall bladder and also a perforation of the gall bladder with suggestion of a large peri-cholecystic collection (Figure 1). At this point duodenoscope was inserted and the using a snare the guideword was pulled out through the channel of the duodenoscope to the outside. An 8 French 20 cm ureteric stent was deployed as a cholecysto-duodenal stent. A ureteric stent was selected for its length and flexibility. This was passed over the guide wire and a 7 French pusher used to push it in place. A combination of guide wire traction and stent grabbing forceps used to ensure accurate positioning (Figure 2 and 3). Subsequently the peri-cholecystic collection was drained with a separate percutaneous drainage placed in the collection (Figure 4). The percutaneous drain dried up over the course of 1 week and was removed under radiological guidance to ensure that the cholecysto-duodenal stent is not disturbed. She has been discharged back to nursing home and will be followed up in out patient’s clinic in due course.
Literature review and Discussion
There have various reports of creation of Cholecysto-duodenal fistula using covered metal stent to treat acute cholecystitis [1–7]. Kumar et al. [1] described a case of empyema of gall bladder with an obstructing hilar cholangiocarcinama preventing bile drainage through the cystic duct. They used multiple metallic stents to drain the biliary tree and created a cholecysto-enteric fistula using covered metal stent. The whole procedure was done using percutaneous radiological guidance. Cholecysto-enteric fistulae have been created using percutaneous technique with radiological guidance [1,2] or endoscopic technique with ultrasound guidance [3–7]. In all these cases a covered metal stent is inserted between the 2 lumens to obtain the desired result. There also have been few reports of trans-papillary drainage of the cholecystitis with perforation of gall bladder [8,9]. However a combined procedure using the technique we have described has not been reported before in the published literature. Our case is also unique as we used a long flexible ureteric stent to overcome short length the stiff architecture of the available CBD stents to achieve this drainage. Simultaneous drainage of peri-cholecystitic collection was also bperfomed. The benefits of our combined approach include minimal manipulation of the papilla and the CBD encountered in trans-papillary route and a perfect positioning of the stent in the gall bladder beyond the impacted stones, which would have difficult to achieve with trans-papillary approach alone. There is no need to create an artificial fistula between the gall bladder and the duodenum thus minimising risks of duodenal leak or bile leak from the puncture site.
Summary
A combined radiological and endoscopic approach has been used for placement of a cholecysto-duodenal stent using an 8 French ureteric stent successfully along with a percutaneous drain to drain the peri-cholecystitis abscess from gall bladder perforation. We have demonstrated that this particular approach is technically feasible and may be indicated in a specific group of patients.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
Keywords
Cholecysto-duodenal; Endoscopic; Ultrasound
Cite this article
Guru Raghavendra GK, Singh S. Cholecysto-duodenal stent using combined percutaneous radiological and endoscopic trans-papillary approach. Clin Surg J. 2021;2(4):1–3.
Copyright
© 2021 Gargeshwari Krishnamurthy Guru Raghavendra. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
