Abstract
Double Aortic Arch (DAA) with an atretic left arch is a rare congenital anomaly. We report a case of double aortic arch with an atretic left arch and retroesophagealligamentum arteriosum in a 5-year-old boy. He underwent successful surgical correction.
Case Presentation
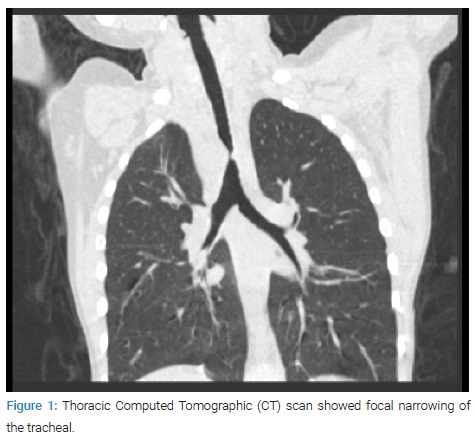
A 5-year-old male child required admission for tachypnea and stridor. The physical examination was unremarkable, and the Electrocardiogram (ECG) was normal. Echocardiography showed right double aortic arch and no intracardiac defects. Thoracic Computed Tomographic (CT) scan showed focal narrowing of the tracheal (Figure 1).
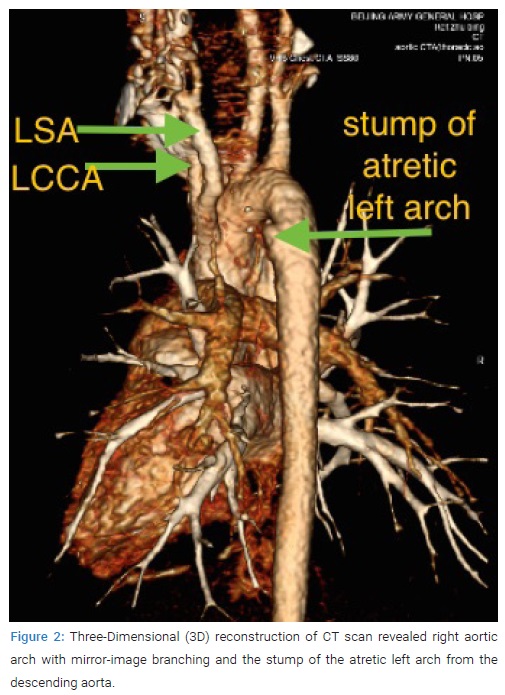
Three-dimensional (3D) reconstruction of CT scan revealed right aortic arch with mirror-image branching and the stump of the atretic left arch from the descending aorta (Figure 2).
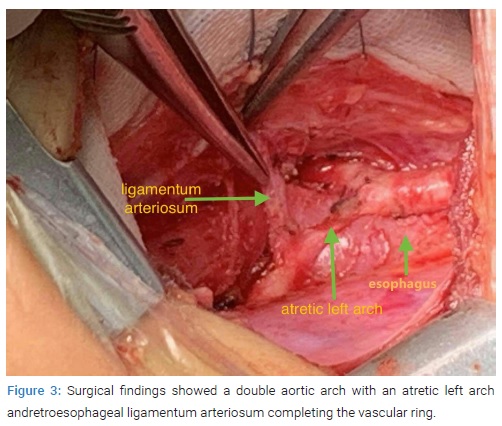
Surgical findings showed a double aortic arch with an atretic left arch and retroesophageal ligamentum arteriosum completing the vascular ring (Figure 3), thus causing compression of trachea and esophagus. Correction of the vascular ring was performed by division and ligation of the atretic left arch and ligamentum arteriosum using a left thoracotomy approach. The patient’s symptom was relieved after surgical correction.
Discussion
Vascular ring is a congenital anomaly in which the aortic arch and its branches completely or incompletely encircle and compress the trachea or esophagus or both [1]. Vascular rings of aortic arch origin account for 1% to 2% of cases of congenital heart disease [2]. Double aortic arch accounts for 50% of vascular rings. Both arches can be equally patent (5%), there is hypoplasia or atresia of the left arch (70%–75%), or the right arch (20%) [3]. Symptoms of vascular ring relate to the consequences of tracheal and esophageal compression [4,5]. Most children with vascular rings present with symptoms within the first several weeks to months of life. The symptoms typically include respiratory distress, stridor, the classic “seal bark” cough, apnea, dysphagia, and recurrent respiratory tract infections [6]. Computed Tomography Angiogram (CTA) is very accurate in the identification of vascular anomalies of the aortic arch and great vessels. However, in some cases the imaging diagnosis by echocardiography (ECHO), CTA or Magnetic Resonance Imaging (MRI) is difficult due to the presence of the atretic segment. In these cases the diagnosis of a complete ring depends on recognizing the arterial branching pattern, the side of the aortic arch, and focal narrowing of the airway [7].
One clue to an arch anomaly is the “four artery sign”which can be seen on sections obtained cephalad to the aortic arch and consists of two dorsal subclavian arteries and two ventral carotid arteries evenly spaced around the trachea [8]. The sign is present when the two dorsal subclavian arteries arise directly from the aortic arch and notfrom a brachiocephalic artery. This occurs with double aortic arches and configurations with aberrant subclavian arteries [9].
To conclude, symptomatic patients should be highly suspicious of vascular ring. The diagnosis of vascular ring can be challenging after ductal closure and arch atresia occurs.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
Keywords
Vascular ring; Double aortic arch; Atretic left aortic arch
Cite this article
Wang G, Zhou G. Double aortic arch with an atretic left arch and retroesophageal ligamentum arteriosum. Clin Surg J. 2021;2(4):1–2.
Copyright
© 2021 Gang Wang. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
