Abstract
This is a case report of 68-year-old lady presented with several months of intermittent epigastric pain and bloating without any relationship to meals. An abdominal computed tomography detected an intussusception at the terminal ileum without proximal obstruction. Subsequent colonoscopy revealed a large caecal tumour with microscopy suggesting diffuse large B-cell lymphoma.The ideal management of solid tumour lymphoma of the bowel is contentious depending on whether the patient is seen by an oncologist or a surgeon and the literature review is not clear on this matter. An oncologist may suggest chemotherapy as the primary treatment, accepting a risk of perforation. However it is the surgeon’s view that the primary treatment should be surgical excision, especially with an anatomical abnormality such as intussusception.
Introduction
A 68-year-old lady presented with several months of intermittent epigastric pain and bloating without any relationship to meals. She had no associated nausea or vomiting, and had regular bowel habits. Clinical examination revealed mild epigastric and right iliac fossa tenderness. A recent colonoscopy complete to the caecum was normal. Abdominal ultrasound and HIDA scan were normal. An abdominal computed tomography detected an intussusception at the terminal ileum without proximal obstruction. No mass lesions were found. Subsequent repeat colonoscopy revealed a large caecal tumour with microscopy suggesting diffuse large B-cell lymphoma. At this stage, a diagnostic laparoscopy also revealed a chronically inflamed gallbladder with significant omental adhesions. After discussion with the patient, and after a multidisciplinary meeting, a laparoscopic cholecystectomy and right hemicolectomy (without reduction) was performed. Intraoperative findings showed a terminal ileal tumour with intussusception into the caecum (Figure 1).

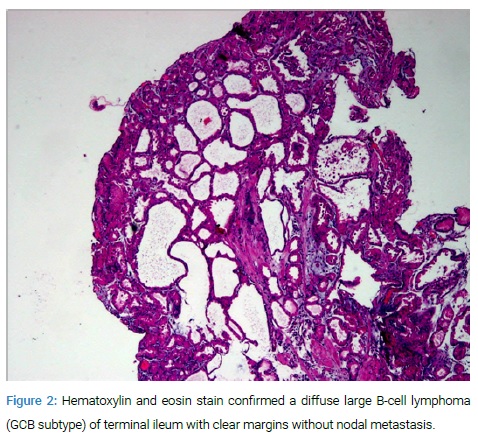
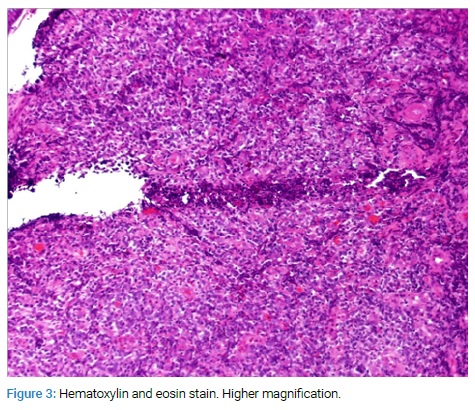
Histopathology confirmed a diffuse large B-cell lymphoma (GCB subtype) of terminal ileum with clear margins without nodal metastasis, and chronic acalculous cholecystitis of the gallbladder (Figure 2 and 3).
The patient was deemed to have Stage 1AE disease and post procedure underwent adjuvant chemotherapy with six cycles of R-CHOP. Follow-up for 3 years reveals no evidence of lymphoma recurrence.
Discussion
Intussusception is a rare condition in adults and represents 1%–5% of total cases of intestinal obstruction. Preoperative diagnosis is even rarer [1]. We report an unusual presentation of a patient with epigastric pain as her primary symptom. In this case, it is likely that her pain was from a combination of her chronic cholecystitis and subacute ileocolic intussusception. Interestingly, the initial colonoscopy did not reveal the tumour, and we feel this was because the level of intussusception was not significant enough for the tumor to protrude into the caecum. A high index of suspicion is needed for intestinal intussusception as symptoms and signs are not pathognomonic, particularly when the aetiology is malignancy [2]. The ideal management of solid tumour lymphoma of the bowel is contentious depending on whether the patient is seen by an oncologist or a surgeon and the literature review is not clear on this matter. An oncologist may suggest chemotherapy as the primary treatment, accepting a risk of perforation. However it is the surgeon’s view that the primary treatment should be surgical excision, especially with an anatomical abnormality such as intussusception.
Conclusion
This case highlights an important point regarding the management of solid tumor bowel lymphomas and whether treatment should be primarily systemic treatment or surgical resection.
Keywords
Epigastric pain; B-cell lymphoma; Intussusception; Caecal tumor
Cite this article
Ratinam R, Duieb Z. To cut or not to cut–that is the question. Intussuscepted B-cell ileal lymphoma. Clin Surg J. 2021;2(1):1–2.
Copyright
© 2021 Ratheesraj Ratinam. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
