Abstract
COVID-19 pandemic is a testing time for every branch of medicine which opened up a new challenge of protecting themselves meantime treating the sick without compromise. For example, treating burns patients, who are very vulnerable for COVID-19 infection. One of the most important step in minimizing the spread of COVID-19 infection is by maintaining social distancing. Now Telemedicine is being revisited as a tool in implementing social distancing, thus providing a safer healthcare. The Telemedicine consultation can be done with Telemedicine Kiosk, hand held devices like smart phone, PTZ camera or drones. The commercially available Telemedicine devices are costly especially Telemedicine Kiosk. Here in this article we are share our experience of using a Telemedicine Kiosk to continue the burns care even during the COVID-19. This Kiosk was made from the materials already available in the department.
Introduction
The COVID-19 is the biggest pandemic world has witnessed in recent time. The healthcare facilities all over the world are working round the clock to provide care to sick. No branch of medicine is left unaffected. For a plastic surgeon working in facility with burns unit, burns patient are most vulnerable, the care of whom cannot be compromised. Meantime he or she also need to protect themselves. The most effective preventive method apart from hand washing and facial mask is to maintain social distance. Telemedicine is being revisited during this pandemic period as a help to plastic surgeons in taking care of vulnerable patients, with the help of information technology. Telemedicine can be a help in providing what is known as ‘healing at a distance’ [1]. Telemedicine is done with digital devices like Kiosk, smart phone, PTZ camera, drones or other hand held devices. For practical purpose Telemedicine can be applied for consultation between doctor and patients, among doctors, between doctor and nurse or between patient and his attenders. But major limiting factor of Telemedicine is commercially available Telemedicine devices are costly. Telemedicine devices are mostly not available in hospitals of developing countries. Though there are cheaper or even free methods to do Telemedicine, such applications are still not popular in developing countries [2,3]. This article shares the experience of using an indigenously made mobile Telemedicine Kiosk and using free video calling applications for Tele-burns ward consultations during lockdown period of COVID-19.
Material and Methods
This study was conducted in the Burns care center of plastic surgery in a tertiary care institution during the COVID-19 pandemic. An Informed consent was taken from all patients and ethical clearance obtained from the departmental ethical committee also prior to study. A Telemedicine Kiosk was made using the material available in the ward (Figure 1), a trolley, an IV stand, a condemned flexible endoscope light source cable was used to mount the Web camera.

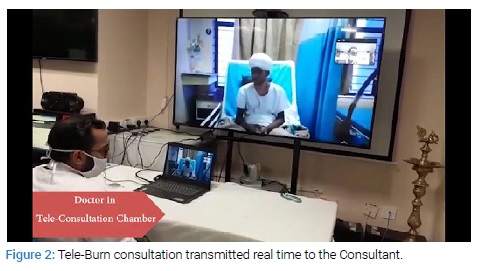
Infrared thermometer, pulse oximeter, digital BP apparatus, digital stethoscope, glucometer, weighing machine, etc. where included in the Kiosk. The Kiosk was connected to free video calling software through institutional Wi-Fi using a laptop. The Kiosk was taken to burns ward and the consultant was present online, resident examined the patient in detail. The resident checked the vitals of patients using the equipment fitted on the Telemedicine Kiosk and findings were conveyed to the consultant Live (Figure 2) and the consultant evaluated the findings and case was discussed. A feedback was taken from the participating doctors about the audio, video and their experience of using the technology and also from the patient.
Results
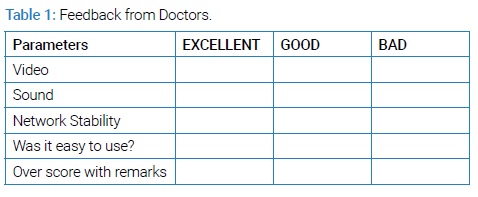
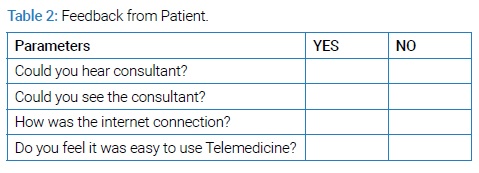
Sample of feedback form (Table 1) the analysis of feedback forms showed that, all the consultations and documents which were shown online were clear. Feedback was also taken from the patients about their experience while talking with the consultants online was found to be satisfactory (Table 2) shows the sample feedback taken from the patients. None of the patients or doctors who attended Telemedicine consultation got infected with COVID-19.
Discussion
Social distancing is the most feasible method to prevent the spread of COVID-19 spread, when and where possible the same should be applied in hospitals also [1–3]. The emergency care or critical patient care cannot be compromised, but the in the treatment of stable patients social distancing can be done to minimize the person to person contact. The information technology tools can be used for communication between patients and doctors or between healthcare workers [4,5]. Based on this principle a Telemedicine Kiosk was made in the department and was used for the Tele-consultations like; Tele-ward rounds, Tele-ICU rounds, Tele-burns ward rounds, Tele-patient-attendant interactions as well as Tele-monitoring of patients or flaps. There are many other ways other than using a Kiosk, like using a mobile phone PTZ camera or drones [6,7]. But advantages of using a Kiosk over other devices are that the Kiosk camera is more static, voice is more clear and most important is while using a Kiosk there is only minimal contact of the equipment with patient or healthcare personal and it can carry all necessary instruments for monitoring the patient. The major disadvantage is larger and space occupying than other devices. There are various video calling application which can be downloaded free of cost like, ZOOM, Google MEET, Skype, WhatsApp, Telegram, etc. they can be used to conduct Tele-consultations. The literature shows that Tele-consultations already being used in developed countries but in developing countries it needs to be made more popular. This study highlights the role of cost-effective Telemedicine.
Conclusion
Telemedicine can play a vital role during COVID-19. And a Telemedicine can be made cost effective.
Keywords
Burns; COVID-19; Tele-consultations
Cite this article
Nishad K, Chittoria RK, Gupta S, Reddy CL, Mohan PB, Pathan I, et al. Mobile telemedicine kiosk for tele-burn ward consultations during COVID-19 period. Clin Surg J. 2020;1(4):1–3.
Copyright
© 2020 Ravi Kumar Chittoria. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
